

Adherence to preventive medications: predictors and outcomes in the Diabetes Prevention Program
- PMID: 16936143
- PMCID: PMC1762037
- DOI: 10.2337/dc06-0454
Adherence to preventive medications: predictors and outcomes in the Diabetes Prevention Program
Abstract
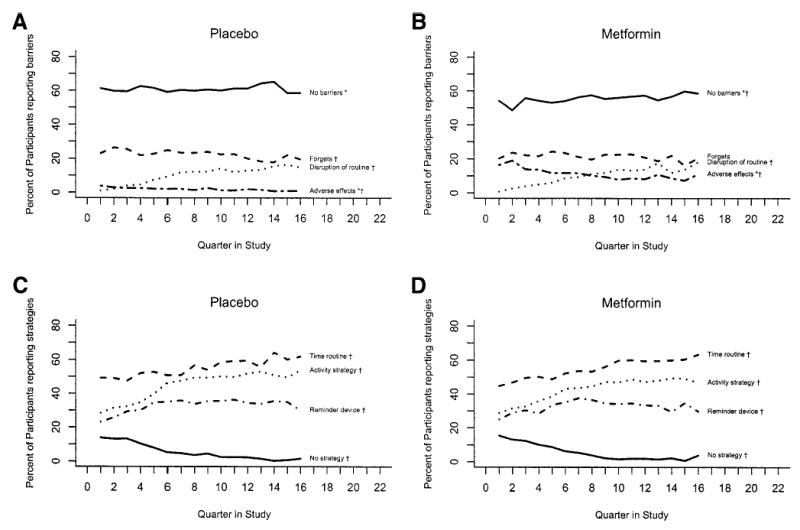
Objective: To evaluate barriers to and strategies for medication adherence and predictors of adherence and the primary outcome in the Diabetes Prevention Program (DPP).
Research design and methods: Within a randomized, controlled primary prevention study for type 2 diabetes, we collected data on study medication adherence, its predictors, and health outcomes in 27 clinical centers across mainland U.S. and Hawaii. Medication arm participants included 2,155 adults with impaired glucose tolerance randomly assigned to either metformin or matched placebo treatment arms. Structured interviews were used to promote medication adherence and to collect data regarding adherence. Adherence was measured by pill count. The primary DPP outcome of type 2 diabetes was assessed by fasting plasma glucose and oral glucose tolerance test.
Results: Older age-groups were more adherent than the youngest group (P = 0.01) in the metformin group. The most frequently reported barrier to adherence was "forgetting" (22%). Women reported more adverse effects of metformin (15 vs. 10%, P = 0.002) in the metformin group. Odds of nonadherence increased as participants reported more than one barrier (odds ratio 19.1, P < 0.001). Odds of adherence increased as participants reported multiple strategies to take medication (2.69, P < 0.0001). There was a 38.2% risk reduction for developing diabetes for those adherent to metformin compared with those adherent to placebo (P < 0.0003).
Conclusions: DPP medication adherence results are unique in primary prevention for a chronic disease in a large multiethnic sample. Our finding that adherence was associated with risk reduction for diabetes supports the development of brief interventions in clinical settings where medication adherence is a challenge.
Figures
References
-
- DiMatteo MR. Variations in patients’ adherence to medical recommendations: a quantitative review of 50 years of research. Med Care. 2004;42:200–209. - PubMed
-
- Dunbar-Jacob J, Erlen JA, Schlenk EA, Ryan CR, Sereika SM, Doswell WM. Adherence in chronic disease. Annu Rev Nurs Res. 2000;18:48–90. - PubMed
-
- Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487–497. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
