

Transhepatic catheter-directed thrombolysis for portal vein thrombosis after partial splenic embolization in combination with balloon-occluded retrograde transvenous obliteration of splenorenal shunt
- PMID: 16937510
- PMCID: PMC4087417
- DOI: 10.3748/wjg.v12.i31.5071
Transhepatic catheter-directed thrombolysis for portal vein thrombosis after partial splenic embolization in combination with balloon-occluded retrograde transvenous obliteration of splenorenal shunt
Abstract
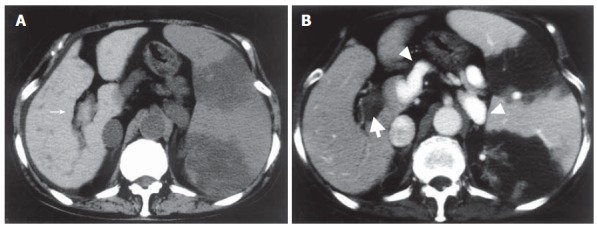
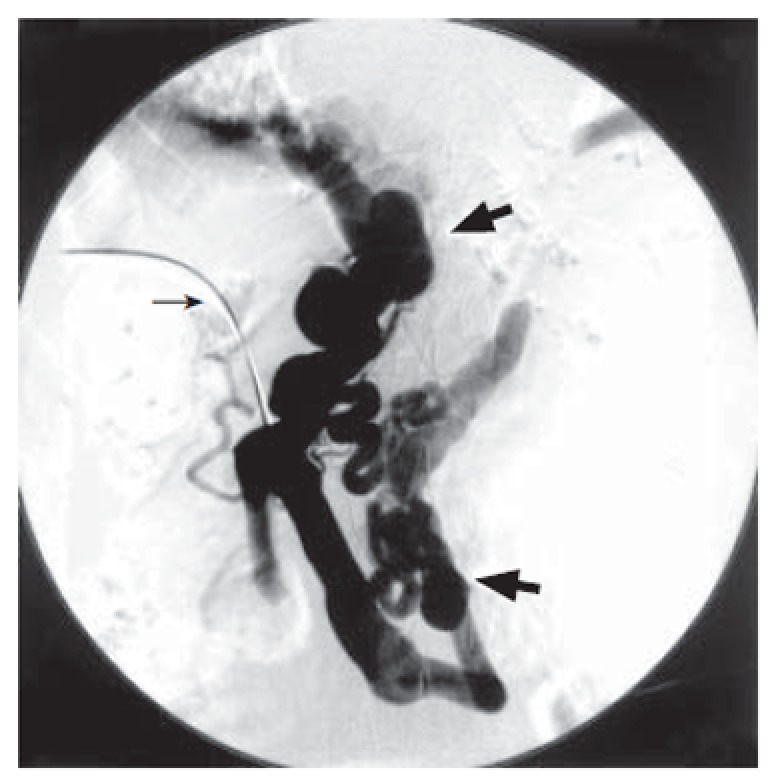
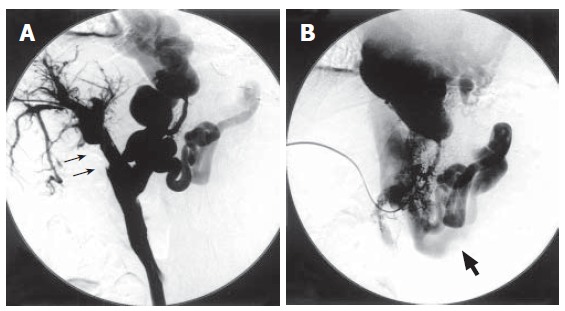
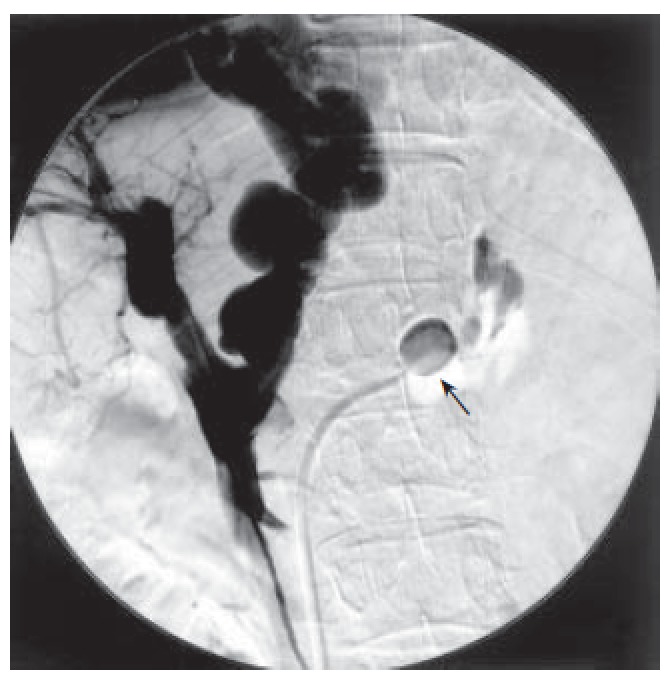
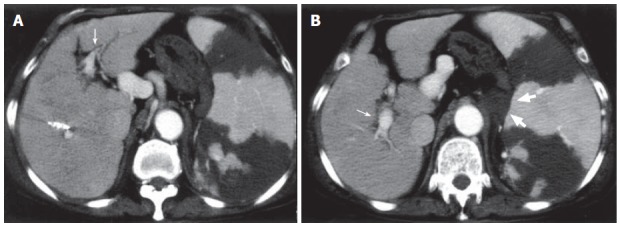
A 66-year-old woman underwent partial splenic embolization (PSE) for hypersplenism with idiopathic portal hypertension (IPH). One week later, contrast-enhanced CT revealed extensive portal vein thrombosis (PVT) and dilated portosystemic shunts. The PVT was not dissolved by the intravenous administration of urokinase. The right portal vein was canulated via the percutaneous transhepatic route under ultrasonic guidance and a 4 Fr. straight catheter was advanced into the portal vein through the thrombus. Transhepatic catheter-directed thrombolysis was performed to dissolve the PVT and a splenorenal shunt was concurrently occluded to increase portal blood flow, using balloon-occluded retrograde transvenous obliteration (BRTO) technique. Subsequent contrast-enhanced CT showed good patency of the portal vein and thrombosed splenorenal shunt. Transhepatic catheter-directed thrombolysis combined with BRTO is feasible and effective for PVT with portosystemic shunts.
Figures
Similar articles
-
Embolization of splenorenal shunt associated to portal vein thrombosis and hepatic encephalopathy.World J Gastroenterol. 2014 Nov 14;20(42):15910-5. doi: 10.3748/wjg.v20.i42.15910. World J Gastroenterol. 2014. PMID: 25400477 Free PMC article.
-
Agitation thrombolysis combined with catheter-directed thrombolysis for the treatment of non-cirrhotic acute portal vein thrombosis.World J Gastroenterol. 2018 Oct 21;24(39):4482-4488. doi: 10.3748/wjg.v24.i39.4482. World J Gastroenterol. 2018. PMID: 30357003 Free PMC article.
-
Portal vein thrombosis after partial splenic embolization in liver cirrhosis: efficacy of anticoagulation and long-term follow-up.J Vasc Interv Radiol. 2013 Dec;24(12):1808-16. doi: 10.1016/j.jvir.2013.08.018. Epub 2013 Oct 4. J Vasc Interv Radiol. 2013. PMID: 24099787
-
Applications of percutaneous mechanical thrombectomy in transjugular intrahepatic portosystemic shunt and portal vein thrombosis.Tech Vasc Interv Radiol. 2003 Mar;6(1):59-69. doi: 10.1053/tvir.2003.36433. Tech Vasc Interv Radiol. 2003. PMID: 12772131 Review.
-
The conventional balloon-occluded retrograde transvenous obliteration procedure: indications, contraindications, and technical applications.Tech Vasc Interv Radiol. 2013 Jun;16(2):101-51. doi: 10.1053/j.tvir.2013.02.003. Tech Vasc Interv Radiol. 2013. PMID: 23830671 Review.
Cited by
-
Embolization of splenorenal shunt associated to portal vein thrombosis and hepatic encephalopathy.World J Gastroenterol. 2014 Nov 14;20(42):15910-5. doi: 10.3748/wjg.v20.i42.15910. World J Gastroenterol. 2014. PMID: 25400477 Free PMC article.
-
Management of acute non-cirrhotic and non-malignant portal vein thrombosis: a systematic review.World J Surg. 2011 Nov;35(11):2510-20. doi: 10.1007/s00268-011-1198-0. World J Surg. 2011. PMID: 21882035
-
Catheter-directed continuous thrombolysis following aspiration thrombectomy via the ileocolic route for acute portal venous thrombosis: report of two cases.Surg Today. 2013 Nov;43(11):1310-5. doi: 10.1007/s00595-012-0343-1. Epub 2012 Sep 25. Surg Today. 2013. PMID: 23007968
-
Management of Spontaneous Portosystemic Shunts in 231 Patients Who Underwent Living Donor Liver Transplantation: A Retrospective Study from a Single Center in Nagasaki, Japan.Ann Transplant. 2022 Aug 23;27:e936371. doi: 10.12659/AOT.936371. Ann Transplant. 2022. PMID: 35996337 Free PMC article.
References
-
- Sangro B, Bilbao I, Herrero I, Corella C, Longo J, Beloqui O, Ruiz J, Zozaya JM, Quiroga J, Prieto J. Partial splenic embolization for the treatment of hypersplenism in cirrhosis. Hepatology. 1993;18:309–314. - PubMed
-
- Romano M, Giojelli A, Capuano G, Pomponi D, Salvatore M. Partial splenic embolization in patients with idiopathic portal hypertension. Eur J Radiol. 2004;49:268–273. - PubMed
-
- N'Kontchou G, Seror O, Bourcier V, Mohand D, Ajavon Y, Castera L, Grando-Lemaire V, Ganne-Carrie N, Sellier N, Trinchet JC, et al. Partial splenic embolization in patients with cirrhosis: efficacy, tolerance and long-term outcome in 32 patients. Eur J Gastroenterol Hepatol. 2005;17:179–184. - PubMed
-
- Eguchi A, Hashizume M, Kitano S, Tanoue K, Wada H, Sugimachi K. High rate of portal thrombosis after splenectomy in patients with esophageal varices and idiopathic portal hypertension. Arch Surg. 1991;126:752–755. - PubMed
-
- Valla DC, Condat B. Portal vein thrombosis in adults: pathophysiology, pathogenesis and management. J Hepatol. 2000;32:865–871. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
