

Randomised study of systematic lymphadenectomy in patients with epithelial ovarian cancer macroscopically confined to the pelvis
- PMID: 16940979
- PMCID: PMC2360519
- DOI: 10.1038/sj.bjc.6603323
Randomised study of systematic lymphadenectomy in patients with epithelial ovarian cancer macroscopically confined to the pelvis
Abstract
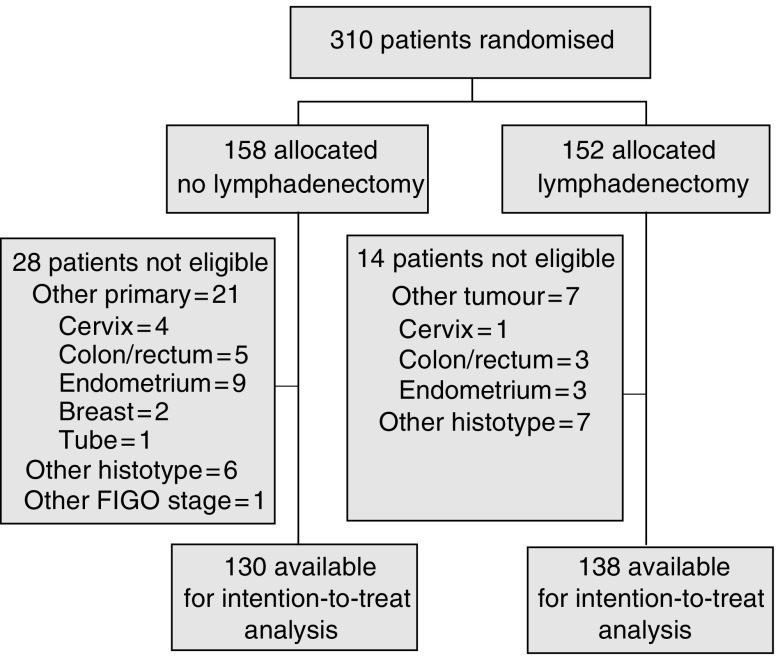
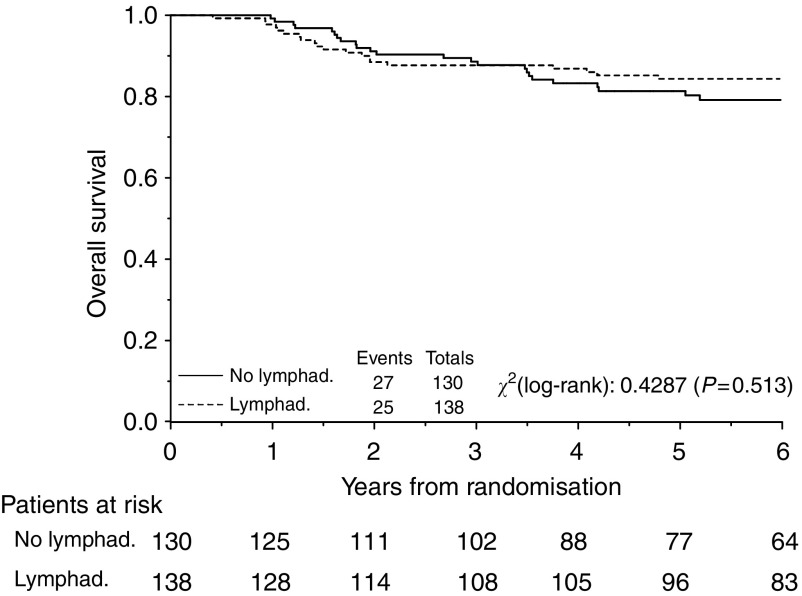
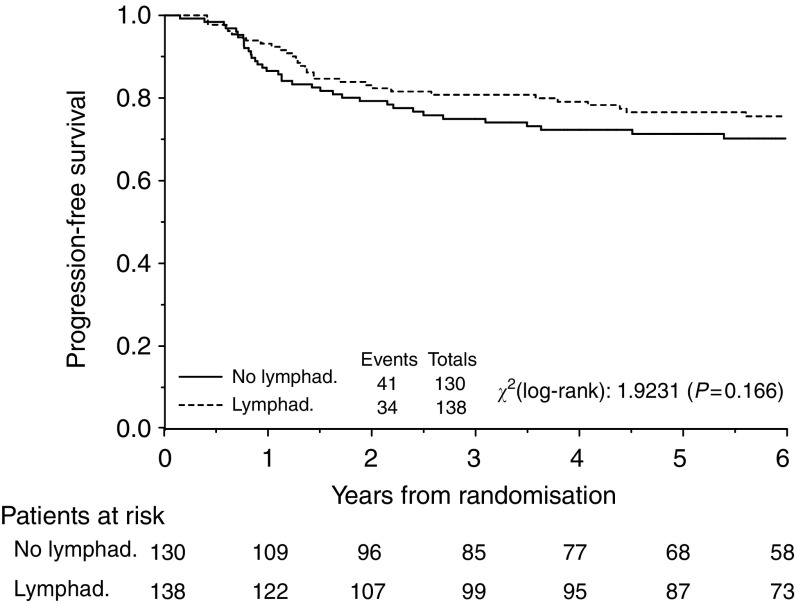
No randomised trials have addressed the value of systematic aortic and pelvic lymphadenectomy (SL) in ovarian cancer macroscopically confined to the pelvis. This study was conducted to investigate the role of SL compared with lymph nodes sampling (CONTROL) in the management of early stage ovarian cancer. A total of 268 eligible patients with macroscopically intrapelvic ovarian carcinoma were randomised to SL (N=138) or CONTROL (N=130). The primary objective was to compare the proportion of patients with retroperitoneal nodal involvement between the two groups. Median operating time was longer and more patients required blood transfusions in the SL arm than the CONTROL arm (240 vs 150 min, P<0.001, and 36 vs 22%, P=0.012, respectively). More patients in the SL group had positive nodes at histologic examination than patients on CONTROL (9 vs 22%, P=0.007). Postoperative chemotherapy was delivered in 66% and 51% of patients with negative nodes on CONTROL and SL, respectively (P=0.03). At a median follow-up of 87.8 months, the adjusted risks for progression (hazard ratio [HR]=0.72, 95%CI=0.46-1.21, P=0.16) and death (HR=0.85, 95%CI=0.49-1.47, P=0.56) were lower, but not statistically significant, in the SL than the CONTROL arm. Five-year progression-free survival was 71.3 and 78.3% (difference=7.0%, 95% CI=-3.4-14.3%) and 5-year overall survival was 81.3 and 84.2% (difference=2.9%, 95% CI=-7.0-9.2%) respectively for CONTROL and SL. SL detects a higher proportion of patients with metastatic lymph nodes. This trial may have lacked power to exclude clinically important effects of SL on progression free and overall survival.
Figures
References
-
- Baiocchi G, Grosso G, Di Re E, Fontanelli R, Raspagliesi F, Di Re F (1998) Systematic pelvic and paraaortic lymphadenectomy at second look laparotomy for ovarian cancer. Gynecol Oncol 69: 151–156 - PubMed
-
- Benedetti Panici P, Greggi S, Maneschi F, Scambia G, Amoroso M, Rabitti C, Mancuso S (1993) Anatomical and pathological study of retroperitoneal nodes in epithelial ovarian cancer. Gynecol Oncol 51: 150–154 - PubMed
-
- Benedetti Panici P, Maggioni A, Hacker N, Landoni F, Ackermann S, Campagnutta E, Tamussino K, Winter R, Pellegrino A, Greggi S, Angioli R, Manci N, Scambia G, Dell'Anna T, Fossati R, Floriani I, Rossi RS, Grassi R, Favalli G, Raspagliesi F, Giannarelli D, Martella L, Mangioni C. (2005) Systematic aortic and pelvic lymphadenectomy vs resection of bulky nodes only in optimally debulked advanced ovarian cancer: a randomised clinical trial. J Natl Cancer Inst 97: 560–566 - PubMed
-
- Burghadt E, Girardi F, Lahousen M, Tamussino K (1991) Patterns of pelvic and paraaortic lymph node involvement in ovarian cancer. Gynecol Oncol 40: 103–106 - PubMed
-
- Carnino F, Fuda G, Ciccone G, Iskra L, Guercio E, Dadone D, Conte PF (1997) Significance of lymph nodes sampling in epithelial carcinoma of the ovary. Gynecol Oncol 65: 467–472 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
