

Serological response to syphilis treatment in HIV-positive and HIV-negative patients attending sexually transmitted diseases clinics
- PMID: 16943224
- PMCID: PMC2598600
- DOI: 10.1136/sti.2006.021402
Serological response to syphilis treatment in HIV-positive and HIV-negative patients attending sexually transmitted diseases clinics
Abstract
Background: HIV-positive patients treated for syphilis may be at increased risk for serological failure.
Objective: To compare follow-up serologies and serological responses to treatment between HIV-positive and HIV-negative patients attending two sexually transmitted disease (STD) clinics.
Study design: Existing records were reviewed from HIV-positive patients who were diagnosed and treated for syphilis at the public STD clinics in Baltimore, Maryland, USA, between 1992 and 2000. Results of their serological follow-up were compared with those of HIV-negative clinic patients at the time of syphilis treatment. Failure was defined as lack of a fourfold drop in rapid plasma reagin (RPR) titre by 400 days after treatment or a fourfold increased titre between 30 and 400 days.
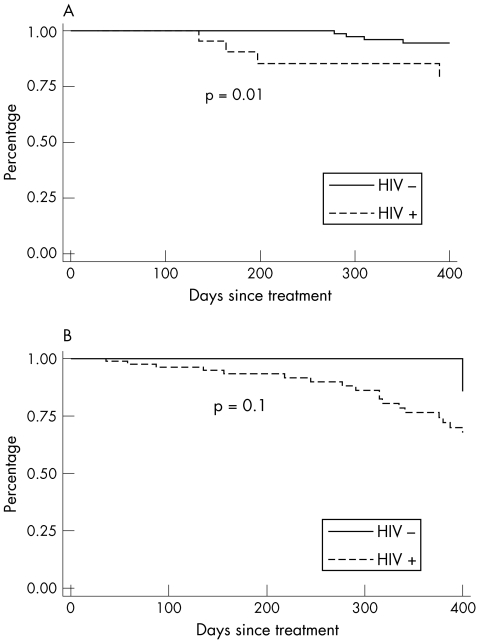
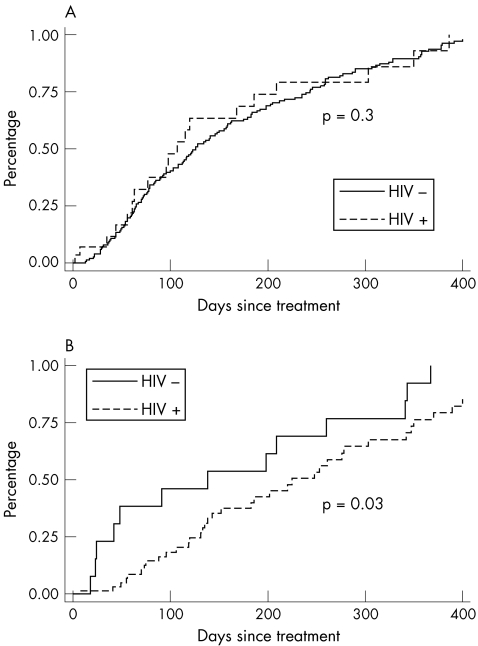
Results: Of the 450 HIV-positive patients with syphilis, 288 (64%) did not have documented follow-up serologies and 129 (28.5%) met the inclusion criteria; 168 (17%) of 1000 known HIV-negative patients were similarly eligible. There were 22 failures in the HIV-positive group and 5 in the HIV-negative group (p<0.001). The median times to successful serological responses in both groups were 278 (95% confidence interval (CI) 209 to 350) and 126 (95% CI 108 to 157) days, respectively (p<0.001). A multivariate Cox's proportional hazards model showed an increased risk of serological failure among the HIV-positive patients (hazards ratio 6.0, 95% CI 1.5 to 23.9; p = 0.01).
Conclusion: HIV-positive patients treated for syphilis may be at higher risk of serological failure. Despite recommendations for more frequent serological follow-up, most patients did not have documentation of serological response after standard treatment for syphilis.
Conflict of interest statement
Competing interests: None.
Similar articles
-
Doxycycline compared with benzathine penicillin for the treatment of early syphilis.Clin Infect Dis. 2006 Mar 15;42(6):e45-9. doi: 10.1086/500406. Epub 2006 Feb 8. Clin Infect Dis. 2006. PMID: 16477545
-
Similar serological response to conventional therapy for syphilis among HIV-positive and HIV-negative women.Genitourin Med. 1995 Oct;71(5):275-9. doi: 10.1136/sti.71.5.275. Genitourin Med. 1995. PMID: 7490041 Free PMC article.
-
The treatment outcome and predictors of serological response in syphilis in a sexually transmitted infections center, China.Int J STD AIDS. 2022 May;33(6):575-583. doi: 10.1177/09564624221086471. Epub 2022 Apr 6. Int J STD AIDS. 2022. PMID: 35384775
-
A systematic review of syphilis serological treatment outcomes in HIV-infected and HIV-uninfected persons: rethinking the significance of serological non-responsiveness and the serofast state after therapy.BMC Infect Dis. 2015 Oct 28;15:479. doi: 10.1186/s12879-015-1209-0. BMC Infect Dis. 2015. PMID: 26511465 Free PMC article.
-
Treatment of syphilis, 1993.Clin Infect Dis. 1995 Apr;20 Suppl 1:S23-38. doi: 10.1093/clinids/20.supplement_1.s23. Clin Infect Dis. 1995. PMID: 7795106 Review.
Cited by
-
Tertiary Syphilis Masquerading as Oropharyngeal Cancer.Cureus. 2022 Sep 7;14(9):e28912. doi: 10.7759/cureus.28912. eCollection 2022 Sep. Cureus. 2022. PMID: 36237821 Free PMC article.
-
Sexually Transmitted Infections Treatment Guidelines, 2021.MMWR Recomm Rep. 2021 Jul 23;70(4):1-187. doi: 10.15585/mmwr.rr7004a1. MMWR Recomm Rep. 2021. PMID: 34292926 Free PMC article.
-
Syphilis and HIV: old and new foes aligned against us.Curr Infect Dis Rep. 2009 Mar;11(2):157-62. doi: 10.1007/s11908-009-0023-5. Curr Infect Dis Rep. 2009. PMID: 19239807
-
Investigating latent syphilis in HIV treatment-experienced Ethiopians and response to therapy.PLoS One. 2022 Jul 12;17(7):e0270878. doi: 10.1371/journal.pone.0270878. eCollection 2022. PLoS One. 2022. PMID: 35819944 Free PMC article. Clinical Trial.
-
Current concepts in bacterial sexually transmitted diseases.Korean J Urol. 2011 Sep;52(9):589-97. doi: 10.4111/kju.2011.52.9.589. Epub 2011 Sep 28. Korean J Urol. 2011. PMID: 22025952 Free PMC article.
References
-
- Blocker M E, Levine W C, St Louis M E. HIV prevalence in patients with syphilis, United States. Sex Transm Dis 20002753–59. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous