

Mahaim fibre tachycardia: recognition and management
Affiliations
- PMID: 16943957
- PMCID: PMC1513516
Item in Clipboard
Mahaim fibre tachycardia: recognition and management
Indian Pacing Electrophysiol J.
.
No abstract available
Figures
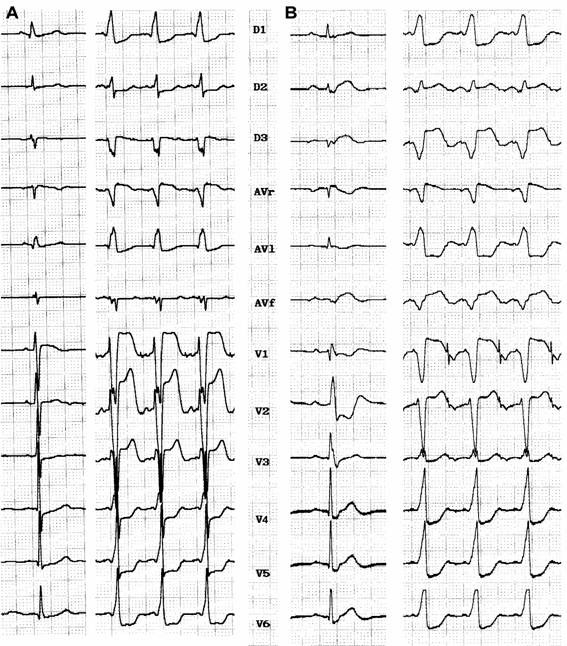
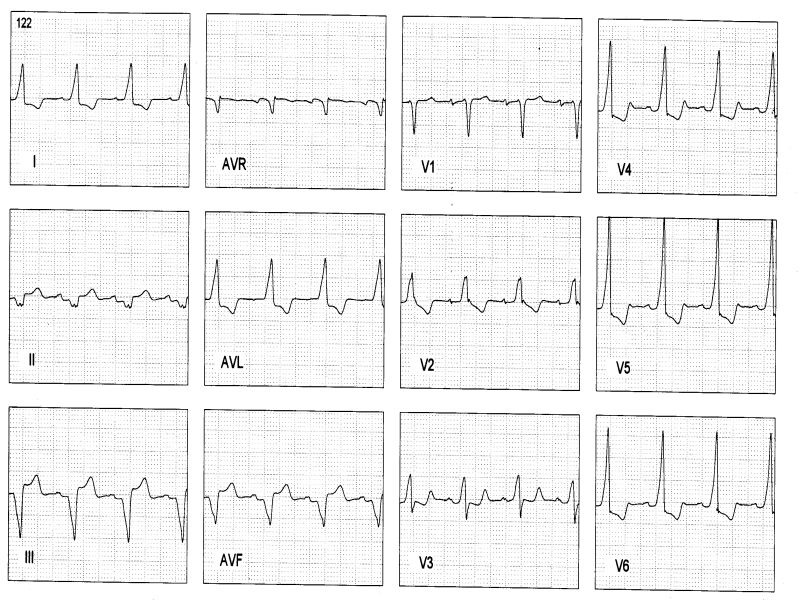
A: Atriofascicular pathway: baseline ECG discloses minimal preexcitation with a 0.12 s PR interval. During atrial pacing LBBB with âQRS= -20°, QRS 130 msec wide. B: Atrioventricular pathway in Ebstein's disease: baseline ECG without preexcitation and disclosing RBBB with normal PR interval. During atrial pacing manifest preexcitation with LBBB (âQRS= -30°), QRS 160 msec wide with a slurred initial r wave in V1
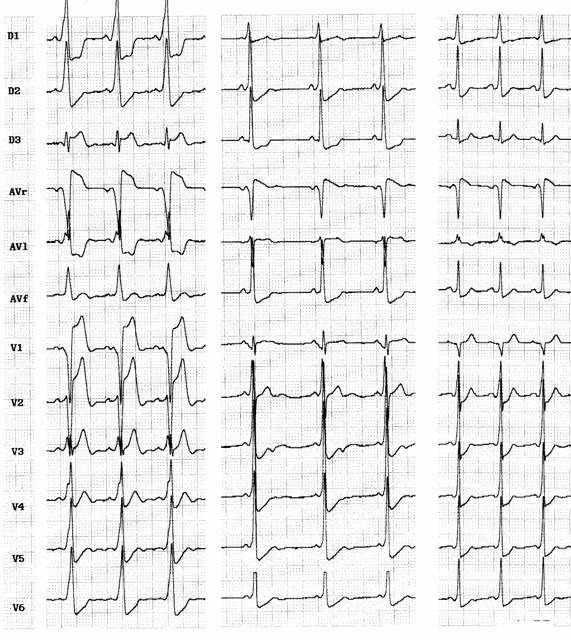
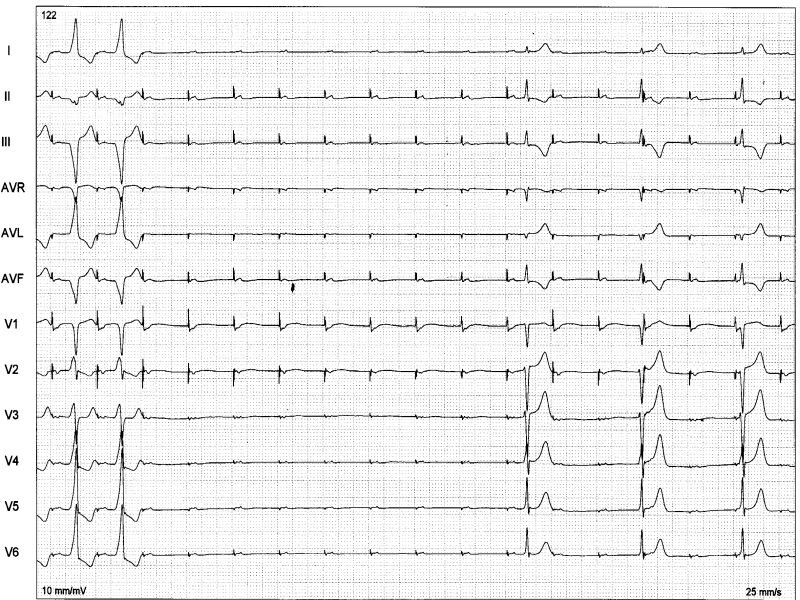
Three cases of fasciculoventricular pathways: PR intervals are 0,08 sec, 0,09 sec and 0,10 sec respectively. QRS is wider in the first ECG and <0.11 sec in the others 2 cases, and frontal plane axis are +30°, +75° and +45°. QRS transition occurs in V3, V2 and V2, respectively.
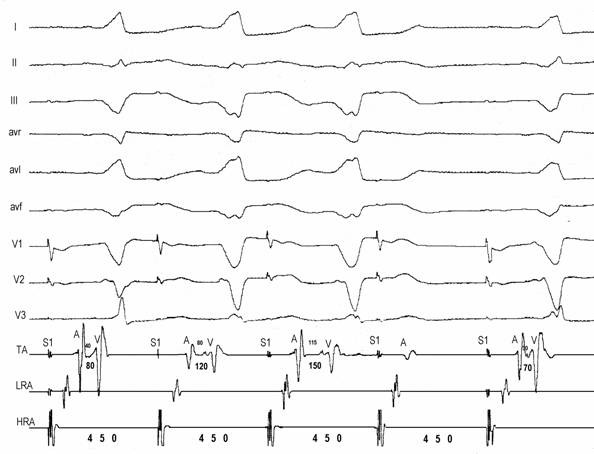
Atrioventricular pathway: high right atrial (HRA) pacing at 450 msec causes Wenckebach block on the accessory pathway. Progressive prolongation of AV interval (80-120-150-block) is due to prolongation of A-AP potential (40-80-115-block). Preexcitation degree increases from the first to the second QRS complex and remains constant in the third QRS despite further prolongation of the A-APP interval.
Antidromic tachycardia. Late (S) atrial extrastimuli delivered from the lateral high right atrium without disturbing AA timing at the His bundle recording advances QRS complex by 20 msec and His deflection by 30 msec, proving that the pathway is extra nodal and participates on the circuit.
Baseline ECG disclosing a normal PR interval (0,16 sec) and a preexcited QRS complex consistent with a right posteroseptal decremental AP
During atrial pacing a brief pulse (1 sec) of radiofrequency current delivered at a site with "M" potential yield a transient complete AV block followed by an escape rhythm without preexcitation (30-35 b/min). Preexcitation resumed in 14 seconds
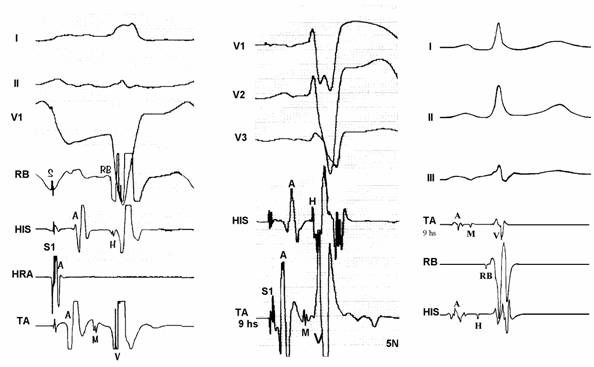
Three examples of "M" potentials (TA- tricuspid annulus electrograms): from left to right: first two cases with His-like potentials and the third with narrow and low amplitude potential. Ablation was successful in each of those sites.
Radiofrequency catheter ablation during atrial pacing: MAT starts immediately after current delivery (RF-ON) and lasted for 8 seconds. Preexcitation is no longer present when MAT terminates.
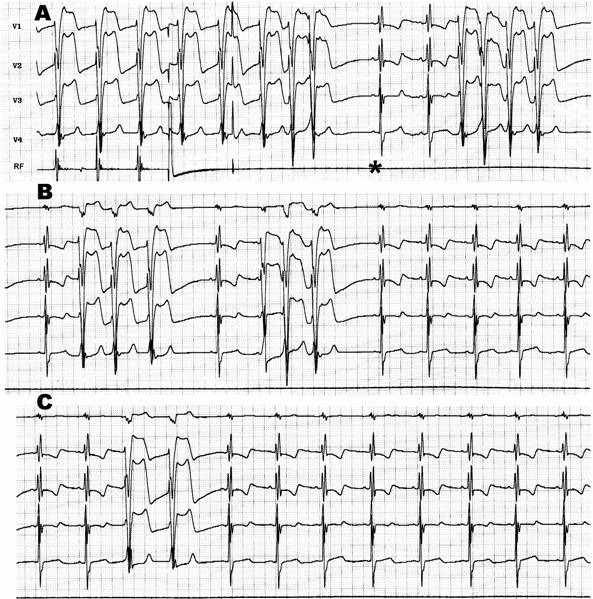
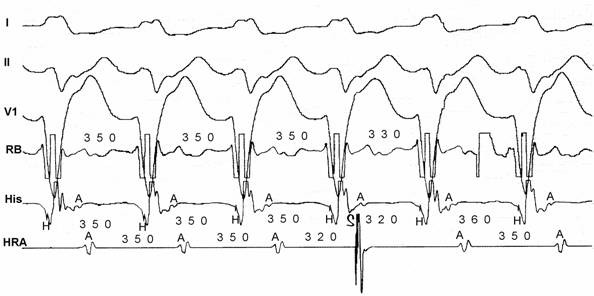
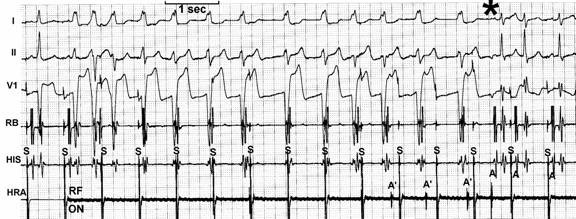
Radiofrequency ablation of recurrent atriofascicular pathway conduction: during ablation salvos of automatic and irregular rhythms with the same QRS morphology as the preexcited one. The salvos persisted even after abolition of preexcitation (*) and fade out until complete disappearance.
Similar articles
-
The automaticity of Mahaim fibre and its response to effective ablation.Chin Med J (Engl). 2004 Dec;117(12):1768-71. Chin Med J (Engl). 2004. PMID: 15603702
-
Electrophysiology study and radiofrequency catheter ablation of atriofascicular tracts with decremental properties (Mahaim fibre) at the tricuspid annulus.Europace. 2008 Dec;10(12):1428-33. doi: 10.1093/europace/eun283. Epub 2008 Oct 19. Europace. 2008. PMID: 18936042 Clinical Trial.
-
Latent Mahaim fiber as a cause of antidromic reciprocating tachycardia: recognition and successful radiofrequency ablation.J Cardiovasc Electrophysiol. 2002 Jan;13(1):74-8. doi: 10.1046/j.1540-8167.2002.00074.x. J Cardiovasc Electrophysiol. 2002. PMID: 11843488
-
Mahaim tachycardias.Eur Heart J. 1998 May;19 Suppl E:E25-31, E52-3. Eur Heart J. 1998. PMID: 9717021 Review.
-
[Mahaim fiber tachycardia and re-entry tachycardia through decremental atrioventricular accessory pathways with anterograde unidirectional block].Cardiologia. 1999 Dec;44 Suppl 1(Pt 1):453-5. Cardiologia. 1999. PMID: 12497951 Review. Italian. No abstract available.
Cited by
-
A single Mahaim accessory pathway with bidirectional delta waves.HeartRhythm Case Rep. 2019 Apr 24;5(7):379-381. doi: 10.1016/j.hrcr.2019.04.004. eCollection 2019 Jul. HeartRhythm Case Rep. 2019. PMID: 31341781 Free PMC article. No abstract available.
-
Not Just a One-Way: Mahaim Accessory Pathway Concomitantly Supporting Orthodromic Atrioventricular Re-Entrant Tachycardia.J Clin Med. 2022 Dec 25;12(1):159. doi: 10.3390/jcm12010159. J Clin Med. 2022. PMID: 36614960 Free PMC article.
-
Comprehensive assessment of Mahaim accessory pathways' anatomic distribution.J Int Med Res. 2022 Jan;50(1):3000605211069751. doi: 10.1177/03000605211069751. J Int Med Res. 2022. PMID: 35001697 Free PMC article.
-
Spontaneous automaticity arising from a successfully ablated Mahaim fiber.J Interv Card Electrophysiol. 2007 Nov;20(1-2):25-8. doi: 10.1007/s10840-007-9164-3. Epub 2007 Oct 18. J Interv Card Electrophysiol. 2007. PMID: 17943429
References
-
- Gallagher JJ, Smith WM, Kassell JH, et al. Role of Mahaim fibers in cardiac arrhythmias in man. Circulation. 1981;64:176–189. - PubMed
-
- Benatt Mahaim I. Nouvelles recherches sur les connexions superiors de la branche gauche du faisceau de His-Tawara avec cloison interventriculaire. Cardiologia. 1938;1:61–120.
-
- Mahaim I. Kent's fibers and the A-V paraspecific conduction through the upper connections of the bundle of His-Tawara. Am Heart J. 1947;33:651. - PubMed
-
- Lev M, Gibson S, Miller RA. Ebstein's disease with Wolff-Parkinson-White syndrome. Am Heart J. 1955;49:724. - PubMed
-
- Becker AE, Anderson RH, Path MRC, et al. The anatomical substrates of Wolff-Parkinson-White syndrome: a clinic-pathologic correlation in seven patients. Circulation. 1978;57:870–879. - PubMed
LinkOut - more resources
Full Text Sources