

Altered creatine kinase adenosine triphosphate kinetics in failing hypertrophied human myocardium
- PMID: 16952984
- PMCID: PMC1808438
- DOI: 10.1161/CIRCULATIONAHA.106.613646
Altered creatine kinase adenosine triphosphate kinetics in failing hypertrophied human myocardium
Abstract
Background: The progression of pressure-overload left ventricular hypertrophy (LVH) to chronic heart failure (CHF) may involve a relative deficit in energy supply and/or delivery.
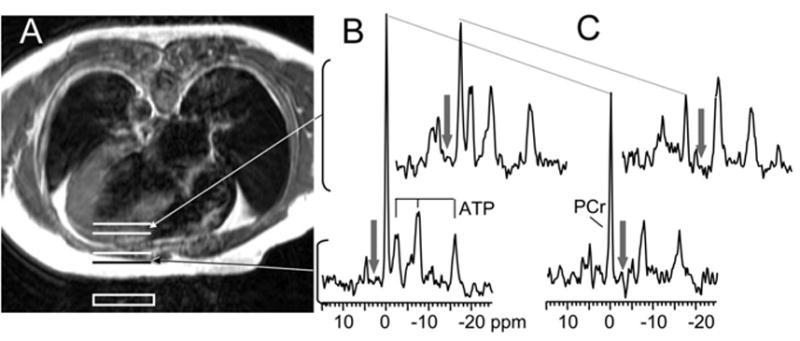
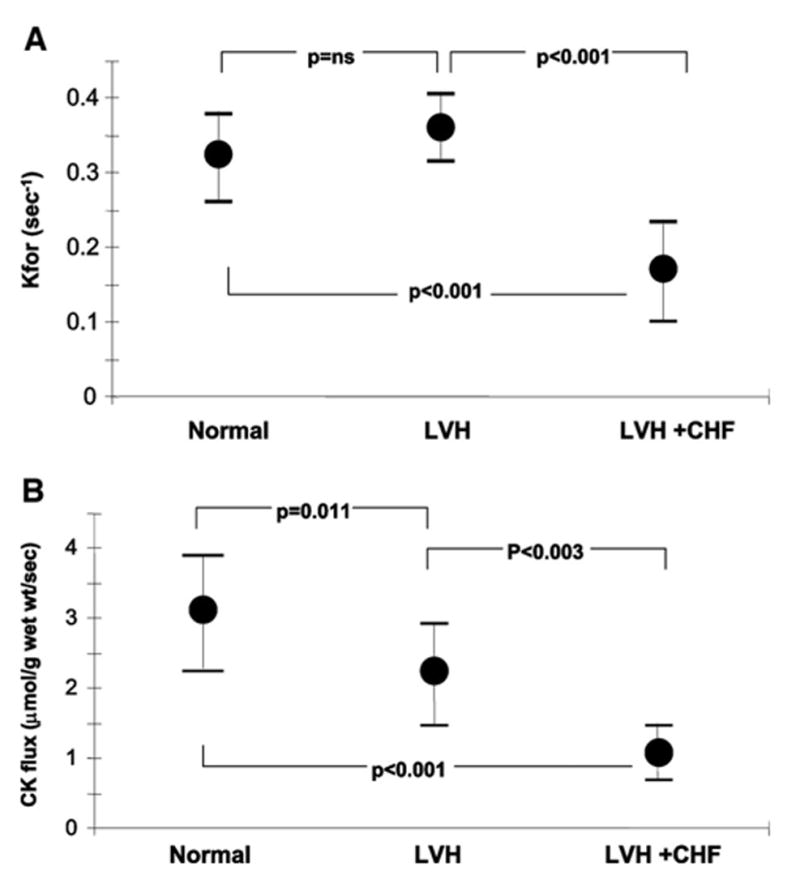
Methods and results: We measured myocardial creatine kinase (CK) metabolite concentrations and adenosine triphosphate (ATP) synthesis through CK, the primary energy reserve of the heart, to test the hypothesis that ATP flux through CK is impaired in patients with LVH and CHF. Myocardial ATP levels were normal, but creatine phosphate levels were 35% lower in LVH patients (n = 10) than in normal subjects (n = 14, P < 0.006). Left ventricular mass and CK metabolite levels in LVH were not different from those in patients with LVH and heart failure (LVH+CHF, n = 10); however, the myocardial CK pseudo first-order rate constant was normal in LVH (0.36 +/- 0.04 s(-1) in LVH versus 0.32 +/- 0.06 s(-1) in normal subjects) but halved in LVH+CHF (0.17 +/- 0.06 s(-1), P < 0.001). The net ATP flux through CK was significantly reduced by 30% in LVH (2.2 +/- 0.7 micromol x g(-1) x s(-1), P = 0.011) and by a dramatic 65% in LVH+CHF (1.1 +/- 0.4 micromol x g(-1) x s(-1), P < 0.001) compared with normal subjects (3.1 +/- 0.8 micromol x g(-1) x s(-1)).
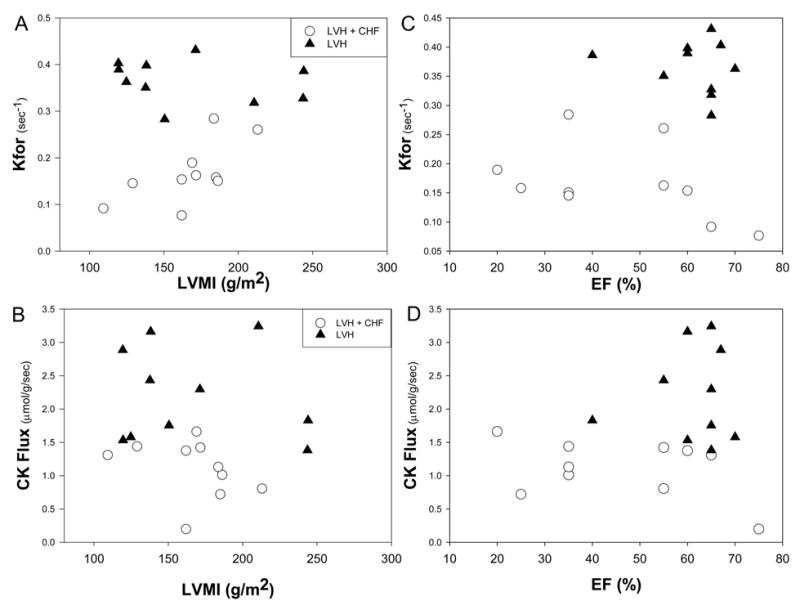
Conclusions: These first observations in human LVH demonstrate that it is not the relative or absolute CK metabolite pool sizes but rather the kinetics of ATP turnover through CK that distinguish failing from nonfailing hypertrophic hearts. Moreover, the deficit in ATP kinetics is similar in systolic and nonsystolic heart failure and is not related to the severity of hypertrophy but to the presence of CHF. Because CK temporally buffers ATP, these observations support the hypothesis that a deficit in myofibrillar energy delivery contributes to CHF pathophysiology in human LVH.
Figures
References
-
- Grossman W. Cardiac hypertrophy: useful adaptation or pathologic process? Am J Med. 1980;69:576–584. - PubMed
-
- Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med. 1990;322:1561–1566. - PubMed
-
- Neely JR, Morgan HE. Relationship between carbohydrate and lipid metabolism and the energy balance of heart muscle. Ann Rev Physiol. 1974;36:413–459. - PubMed
-
- Ingwall JS, Kramer MF, Fifer MA, Lorell BH, Shemin R, Grossman W, Allen PD. The creatine kinase system in normal and diseased human myocardium. N Engl J Med. 1985;313:1050–1054. - PubMed
-
- Wallimann T. Bioenergetics: dissecting the role of creatine kinase. Curr Biol. 1994;4:42–46. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
