

An experimental model of rhinovirus induced chronic obstructive pulmonary disease exacerbations: a pilot study
- PMID: 16956406
- PMCID: PMC1578567
- DOI: 10.1186/1465-9921-7-116
An experimental model of rhinovirus induced chronic obstructive pulmonary disease exacerbations: a pilot study
Abstract
Background: Acute exacerbations of COPD are a major cause of morbidity, mortality and hospitalisation. Respiratory viruses are associated with the majority of exacerbations but a causal relationship has not been demonstrated and the mechanisms of virus-induced exacerbations are poorly understood. Development of a human experimental model would provide evidence of causation and would greatly facilitate understanding mechanisms, but no such model exists.
Methods: We aimed to evaluate the feasibility of developing an experimental model of rhinovirus induced COPD exacerbations and to assess safety of rhinovirus infection in COPD patients. We carried out a pilot virus dose escalating study to assess the minimum dose of rhinovirus 16 required to induce experimental rhinovirus infection in subjects with COPD (GOLD stage II). Outcomes were assessed by monitoring of upper and lower respiratory tract symptoms, lung function, and virus replication and inflammatory responses in nasal lavage.
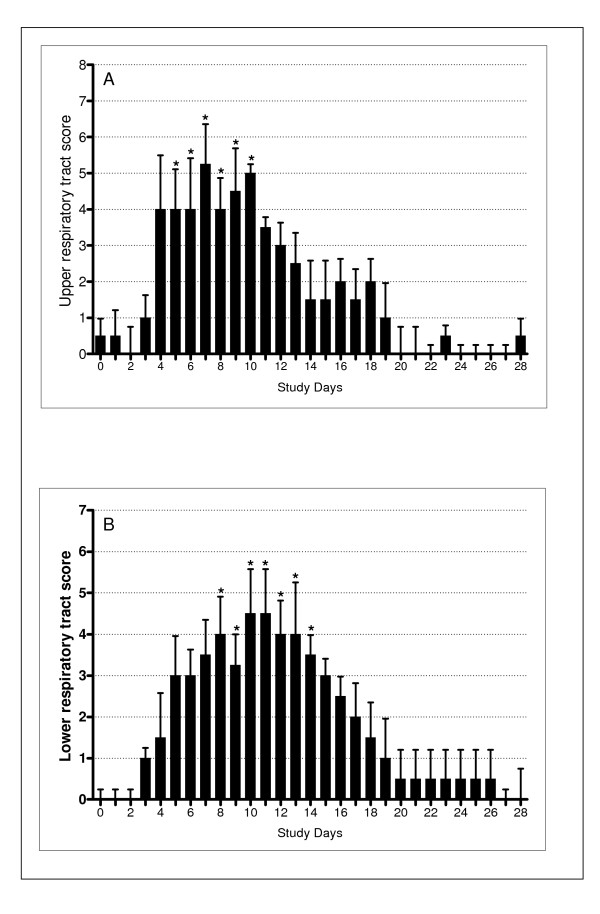
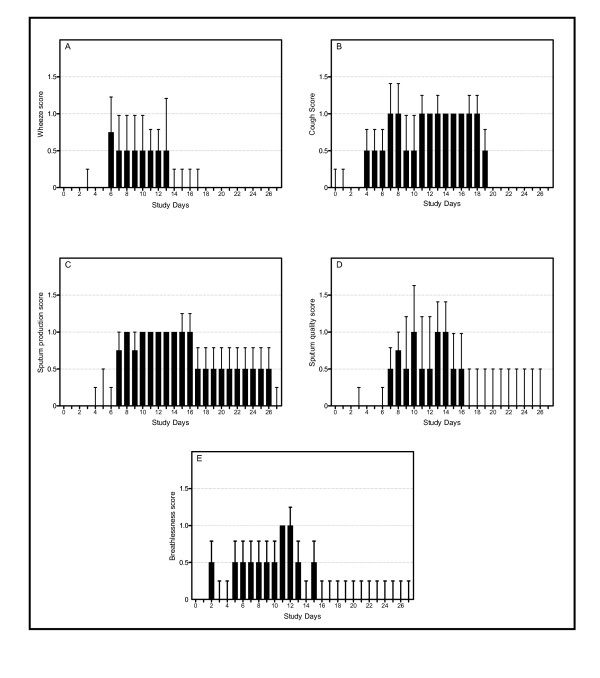
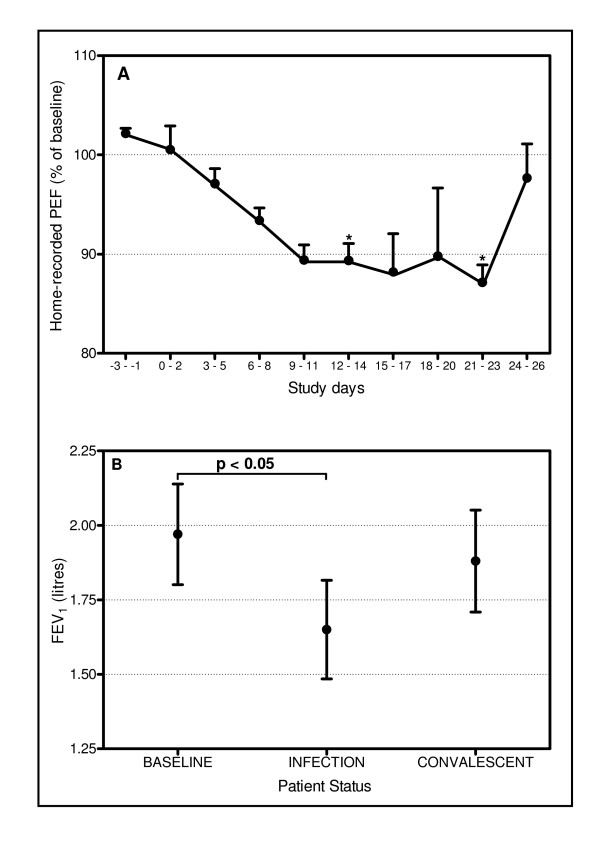
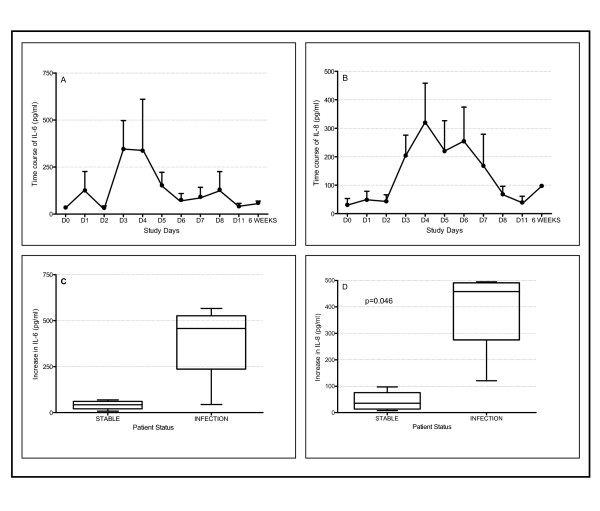
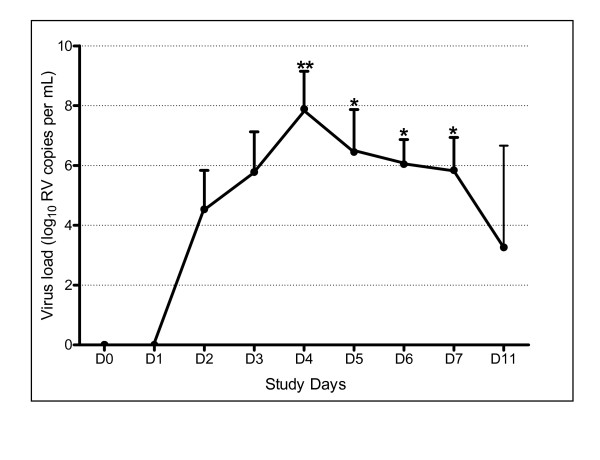
Results: All 4 subjects developed symptomatic colds with the lowest dose of virus tested, associated with evidence of viral replication and increased pro-inflammatory cytokines in nasal lavage. These were accompanied by significant increases in lower respiratory tract symptoms and reductions in PEF and FEV1. There were no severe exacerbations or other adverse events.
Conclusion: Low dose experimental rhinovirus infection in patients with COPD induces symptoms and lung function changes typical of an acute exacerbation of COPD, appears safe, and provides preliminary evidence of causation.
Figures
References
-
- Anthonisen NR, Manfreda J, Warren CP, Hershfield ES, Harding GK, Nelson NA. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Annals of Internal Medicine. 1987;106:196–204. - PubMed
-
- Seemungal T, Harper-Owen R, Bhowmik A, Moric I, Sanderson G, Message S, Maccallum P, Meade TW, Jeffries DJ, Johnston SL, Wedzicha JA. Respiratory viruses, symptoms, and inflammatory markers in acute exacerbations and stable chronic obstructive pulmonary disease. [see comments.] American Journal of Respiratory & Critical Care Medicine. 2001;164:1618–1623. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
