

Incidence and causes of severe neonatal hyperbilirubinemia in Canada
- PMID: 16966660
- PMCID: PMC1559442
- DOI: 10.1503/cmaj.060328
Incidence and causes of severe neonatal hyperbilirubinemia in Canada
Abstract
Background: Severe hyperbilirubinemia is the most common cause of neonatal readmission to hospital in Canada even though, in the majority of cases, risk factors can be identified before discharge. Severe neonatal hyperbilirubinemia and kernicterus continue to be reported worldwide in otherwise healthy term infants. We conducted this study to estimate the incidence of severe neonatal hyperbilirubinemia in Canada and to determine underlying causes, improved knowledge of which would be valuable to help identify strategies for risk reduction.
Methods: Data on term infants 60 days of age and younger with unconjugated hyperbilirubinemia were collected prospectively through the Canadian Paediatric Surveillance Program from 2002 to 2004. Infants were included if they had a peak serum total bilirubin level of more than 425 micromol/L or underwent an exchange transfusion. Infants with rhesus iso-immunization or who were born at less than 36 weeks' gestation were excluded.
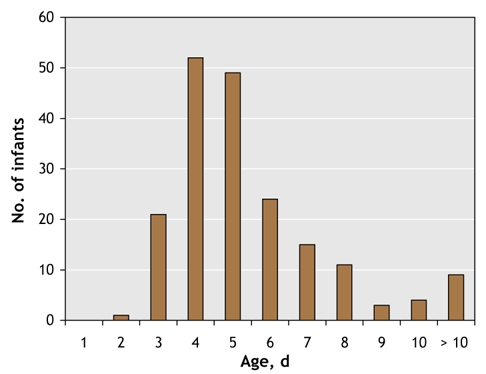
Results: Of 367 cases reported, 258 were confirmed to be severe neonatal hyperbilirubinemia, for an estimated incidence of 1 in 2480 live births. Causes were identified in 93 cases and included ABO incompatibility (n = 48), glucose-6-phosphate dehydrogenase deficiency (n = 20), other antibody incompatibility (n = 12) and hereditary spherocytosis (n = 7). The mean peak bilirubin level reported was 471 micromol/L (standard deviation [SD] 76 micromol/L, range 156-841 micromol/L). Fifty-seven infants (22.1%) underwent an exchange transfusion. A total of 185 infants (71.7%) were readmitted to hospital, 121 (65.4%) of them within 5 days of age.
Interpretation: Severe neonatal hyperbilirubinemia continues to occur frequently in Canada. In the majority of cases, the underlying cause was not identified. The high readmission rate within days after initial discharge indicates a need for a more thorough assessment of newborn infants and consideration of strategies to identify at-risk newborns, such as predischarge measurement of serum bilirubin levels.
Figures
Comment in
-
Surveillance of severe neonatal hyperbilirubinemia: a view from south of the border.CMAJ. 2006 Sep 12;175(6):599. doi: 10.1503/cmaj.060960. CMAJ. 2006. PMID: 16966662 Free PMC article. No abstract available.
-
Coombs' testing and neonatal hyperbilirubinemia.CMAJ. 2007 Mar 27;176(7):972-3; author reply 973. doi: 10.1503/cmaj.1060214. CMAJ. 2007. PMID: 17389451 Free PMC article. No abstract available.
References
-
- Tan-Dy C, Moore A, Satodia P, et al. Predicting kernicterus in severe unconjugated hyperbilirubinemia. Paediatr Child Health 2004;9(Suppl A):17A.
-
- Lee K, Perlman M. The impact of early obstetric discharge on newborn health care. Curr Opin Pediatr 1996;8:96-101. - PubMed
-
- Lee K, Perlman M, Ballantyne M, et al. Association between duration of neonatal hospital stay and readmission rate. J Pediatr 1995;127:758-66. - PubMed
-
- Brown AK, Damusk K, Kim MH, et al. Factors relating to readmission of term and near-term neonates in the first two weeks of life. J Perinat Med 1999;27:263-75. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources