

Benefit design and specialty drug use
- PMID: 16966729
- PMCID: PMC6349207
- DOI: 10.1377/hlthaff.25.5.1319
Benefit design and specialty drug use
Abstract
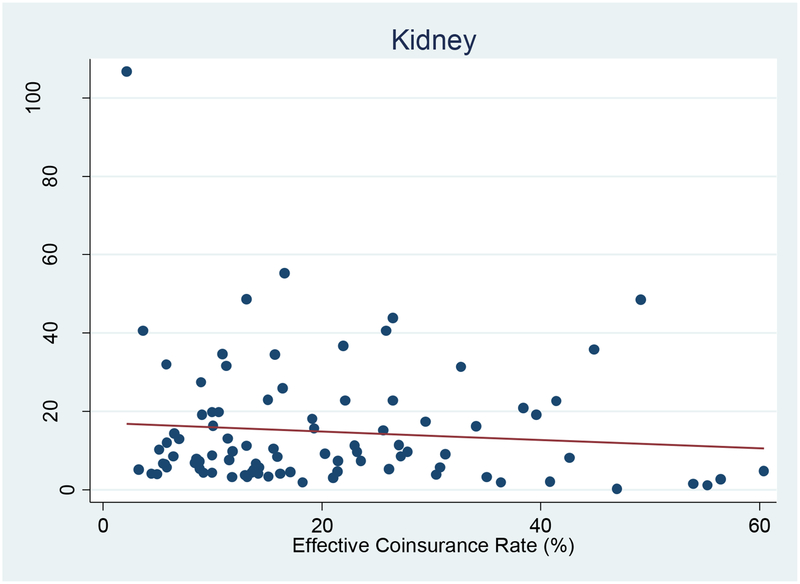
In this paper we examine spending by privately insured patients with four conditions often treated with specialty drugs: cancer, kidney disease, rheumatoid arthritis, and multiple sclerosis. Despite having employer-sponsored health insurance, these patients face substantial risk for high out-of-pocket spending. In contrast to traditional pharmaceuticals, we find that specialty drug use is largely insensitive to cost sharing, with price elasticities ranging from 0.01 to 0.21. Given the expense of many specialty drugs, care management should focus on making sure that patients who will most benefit receive them. Once such patients are identified, it makes little economic sense to limit coverage.
Figures
References
-
- Smith C, Cowan C, Heffler S, Catlin A, NHAT, “National Health Spending In 2004: Recent Slowdown Led By Prescription Drug Spending,” Health Affairs, 2006, Vol. 25, No. 1, pp. 186–196. - PubMed
-
-
Specialty Pharmacy News, January 2004.
-
-
-
Technical Appendix.
-
-
-
Not every health plan was available in both years; in total there were 91 plan-years.
-
-
-
The cause of anemia cannot be ascertained in claims data so all patients with anemia are included in this category. This aggregation is consistent given that specialty drugs used to treat anemia also do not vary with underlying disease. Sensitivity analysis demonstrated that the subsequent elasticities are similar when anemia patients are excluded.
-
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical