

Feasibility and cost-effectiveness of treating multidrug-resistant tuberculosis: a cohort study in the Philippines
- PMID: 16968123
- PMCID: PMC1564168
- DOI: 10.1371/journal.pmed.0030352
Feasibility and cost-effectiveness of treating multidrug-resistant tuberculosis: a cohort study in the Philippines
Abstract
Background: Multidrug-resistant tuberculosis (MDR-TB) is an important global health problem, and a control strategy known as DOTS-Plus has existed since 1999. However, evidence regarding the feasibility, effectiveness, cost, and cost-effectiveness of DOTS-Plus is still limited.
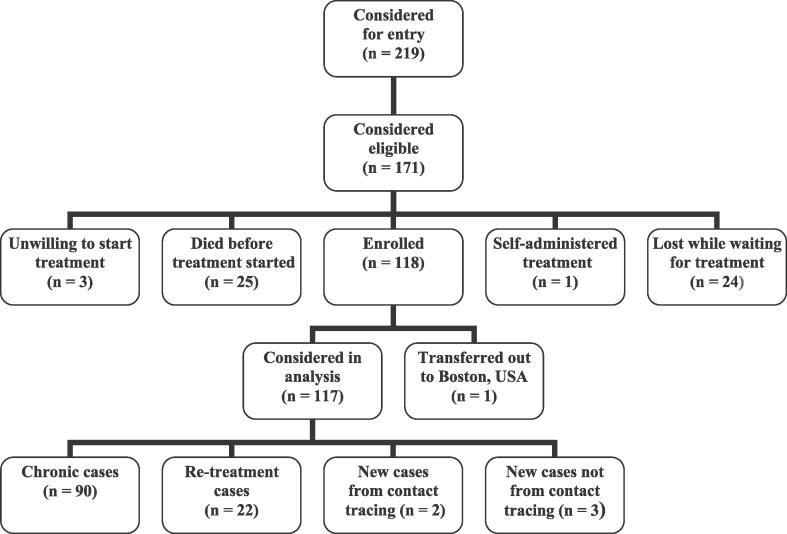
Methodology/principal findings: We evaluated the feasibility, effectiveness, cost, and cost-effectiveness of a DOTS-Plus pilot project established at Makati Medical Center in Manila, the Philippines, in 1999. Patients with MDR-TB are treated with regimens, including first- and second-line drugs, tailored to their drug susceptibility pattern (i.e., individualised treatment). We considered the cohort enrolled between April 1999 and March 2002. During this three-year period, 118 patients were enrolled in the project; 117 were considered in the analysis. Seventy-one patients (61%) were cured, 12 (10%) failed treatment, 18 (15%) died, and 16 (14%) defaulted. The average cost per patient treated was US3,355 dollars from the perspective of the health system, of which US1,557 dollars was for drugs, and US837 dollars from the perspective of patients. The mean cost per disability-adjusted life year (DALY) gained by the DOTS-Plus project was US242 dollars (range US85 dollars to US426 dollars).
Conclusions: Treatment of patients with MDR-TB using the DOTS-Plus strategy and individualised drug regimens can be feasible, comparatively effective, and cost-effective in low- and middle-income countries.
Conflict of interest statement
Figures
Comment in
-
Is DOTS-plus a feasible and cost-effective strategy?PLoS Med. 2006 Sep;3(9):e350. doi: 10.1371/journal.pmed.0030350. PLoS Med. 2006. PMID: 16968122 Free PMC article. Review.
-
Multidrug-resistant TB in the Philippines: totem and taboo.PLoS Med. 2006 Dec;3(12):e539; author reply e549. doi: 10.1371/journal.pmed.0030539. PLoS Med. 2006. PMID: 17194204 Free PMC article. No abstract available.
References
-
- Espinal MA, Laszlo A, Simonsen L, Boulahbal F, Kim SJ, et al. Global trends in resistance to antituberculosis drugs. New Engl J Med. 2001;344:1294–1303. - PubMed
-
- Pablos-Mendez A, Raviglione MC, Laszlo A, Binkin N, Rieder HL, et al. Global surveillance for antituberculosis-drug resistance, 1994−1997. World Health Organization—International Union against Tuberculosis and Lung Disease Working Group on Anti-Tuberculosis Drug Resistance Surveillance. New Engl J Med. 1998;338:1641–1649. - PubMed
-
- World Health Organization, IUATLD. Anti-tuberculosis drug resistance in the world: The WHO/IUATLD Global Project on Anti-Tuberculosis Drug Resistance Surveillance Report No. 3. Geneva: WHO; 2004.
-
- World Health Organization. Global tuberculosis control: Surveillance, planning, financing. WHO/HTM/TB/2006.362. WHO: Geneva; 2006.
-
- Espinal M, Kim SJ, Suarez P, Kam KM, Khomenko AG, et al. Standard short-course chemotherapy for drug resistant tuberculosis. Treatment outcomes in six countries. JAMA. 2003;283:2537–2545. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
