

Meta-analysis: anticholinergics, but not beta-agonists, reduce severe exacerbations and respiratory mortality in COPD
- PMID: 16970553
- PMCID: PMC1831628
- DOI: 10.1111/j.1525-1497.2006.00507.x
Meta-analysis: anticholinergics, but not beta-agonists, reduce severe exacerbations and respiratory mortality in COPD
Erratum in
- J Gen Intern Med. 2006 Oct;21(10):1131
Abstract
Background: Anticholinergics and beta2-agonists have generally been considered equivalent choices for bronchodilation in chronic obstructive pulmonary disease (COPD).
Objective: To assess the safety and efficacy of anticholinergics and beta2-agonists in COPD.
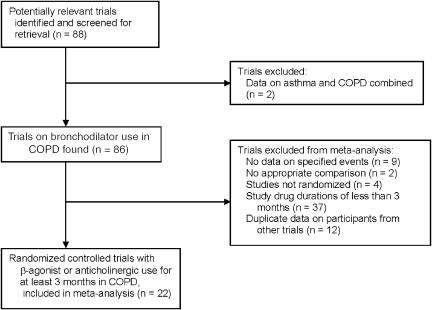
Design: We comprehensively searched electronic databases from 1966 to December 2005, clinical trial websites, and references from selected reviews. We included randomized controlled trials of at least 3 months duration that evaluated anticholinergic or beta2-agonist use compared with placebo or each other in patients with COPD.
Measurements: We evaluated the relative risk (RR) of exacerbations requiring withdrawal from the trial, severe exacerbations requiring hospitalization, and deaths attributed to a lower respiratory event.
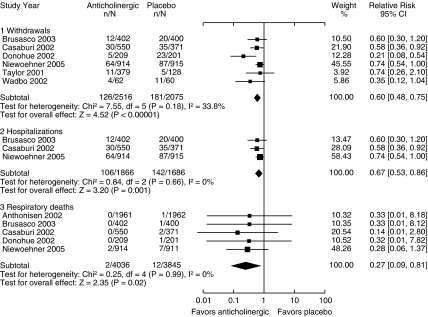
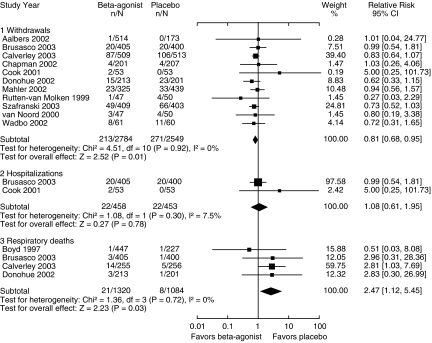
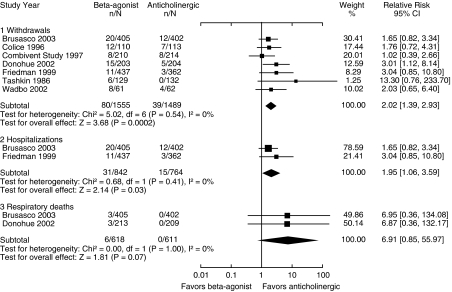
Results: Pooled results from 22 trials with 15,276 participants found that anticholinergic use significantly reduced severe exacerbations (RR 0.67, confidence interval [CI] 0.53 to 0.86) and respiratory deaths (RR 0.27, CI 0.09 to 0.81) compared with placebo. Beta2-agonist use did not affect severe exacerbations (RR 1.08, CI 0.61 to 1.95) but resulted in a significantly increased rate of respiratory deaths (RR 2.47, CI 1.12 to 5.45) compared with placebo. There was a 2-fold increased risk for severe exacerbations associated with beta2-agonists compared with anticholinergics (RR 1.95, CI 1.39 to 2.93). The addition of beta2-agonist to anticholinergic use did not improve any clinical outcomes.
Conclusion: Inhaled anticholinergics significantly reduced severe exacerbations and respiratory deaths in patients with COPD, while beta2-agonists were associated with an increased risk for respiratory deaths. This suggests that anticholinergics should be the bronchodilator of choice in patients with COPD, and beta2-agonists may be associated with worsening of disease control.
Figures
Comment in
-
Time to question long-term safety of routine scheduled inhaled beta-2-agonist treatment for COPD.J Gen Intern Med. 2006 Oct;21(10):1123-4. doi: 10.1111/j.1525-1497.2006.00602.x. J Gen Intern Med. 2006. PMID: 16970562 Free PMC article. No abstract available.
-
Review: anticholinergics, but not beta2-agonists, reduce exacerbations requiring hospitalization and respiratory deaths in COPD.ACP J Club. 2007 Jan-Feb;146(1):19. ACP J Club. 2007. PMID: 17203939 No abstract available.
-
Review: anticholinergics but not beta2 agonists reduce exacerbations requiring hospital admission and respiratory deaths in COPD.Evid Based Med. 2007 Feb;12(1):13. doi: 10.1136/ebm.12.1.13. Evid Based Med. 2007. PMID: 17264261 No abstract available.
-
Effects of anticholinergics and beta-agonists in COPD.J Gen Intern Med. 2007 Jun;22(6):893; author reply 894. doi: 10.1007/s11606-006-0096-x. J Gen Intern Med. 2007. PMID: 17406953 Free PMC article. No abstract available.
References
-
- Celli BR, MacNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23:932–46. - PubMed
-
- Agusti AG. COPD, a multicomponent disease: implications for management. Respir Med. 2005;99:670–82. - PubMed
-
- McCrory DC, Brown CD, Gelfand SE, Bach PB. Management of acute exacerbations of COPD A summary and appraisal of published evidence. Chest. 2001;119:1190–209. - PubMed
-
- U.S. Department of Health and Human Services. COPD data fact sheet. 2003. NIH publication No. 03-5229.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical