

Changes in aortic blood flow induced by passive leg raising predict fluid responsiveness in critically ill patients
- PMID: 16970817
- PMCID: PMC1751046
- DOI: 10.1186/cc5044
Changes in aortic blood flow induced by passive leg raising predict fluid responsiveness in critically ill patients
Abstract
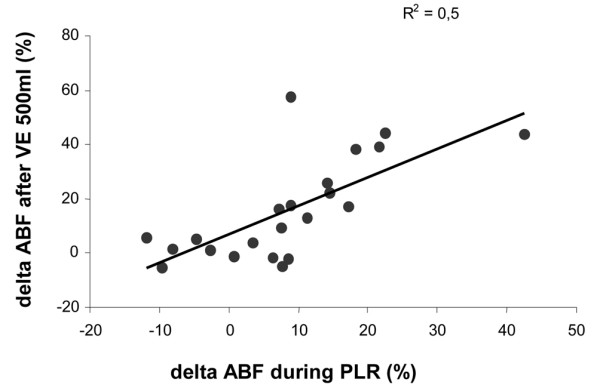
Introduction: Esophageal Doppler provides a continuous and non-invasive estimate of descending aortic blood flow (ABF) and corrected left ventricular ejection time (LVETc). Considering passive leg raising (PLR) as a reversible volume expansion (VE), we compared the relative abilities of PLR-induced ABF variations, LVETc and respiratory pulsed pressure variations (DeltaPP) to predict fluid responsiveness.
Methods: We studied 22 critically ill patients in acute circulatory failure in the supine position, during PLR, back to the supine position and after two consecutive VEs of 250 ml of saline. Responders were defined by an increase in ABF induced by 500 ml VE of more than 15%.
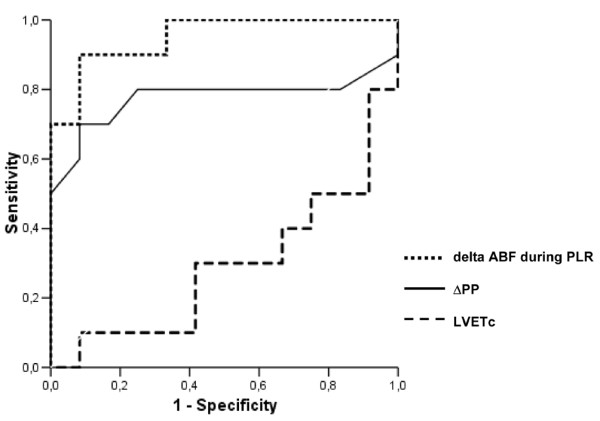
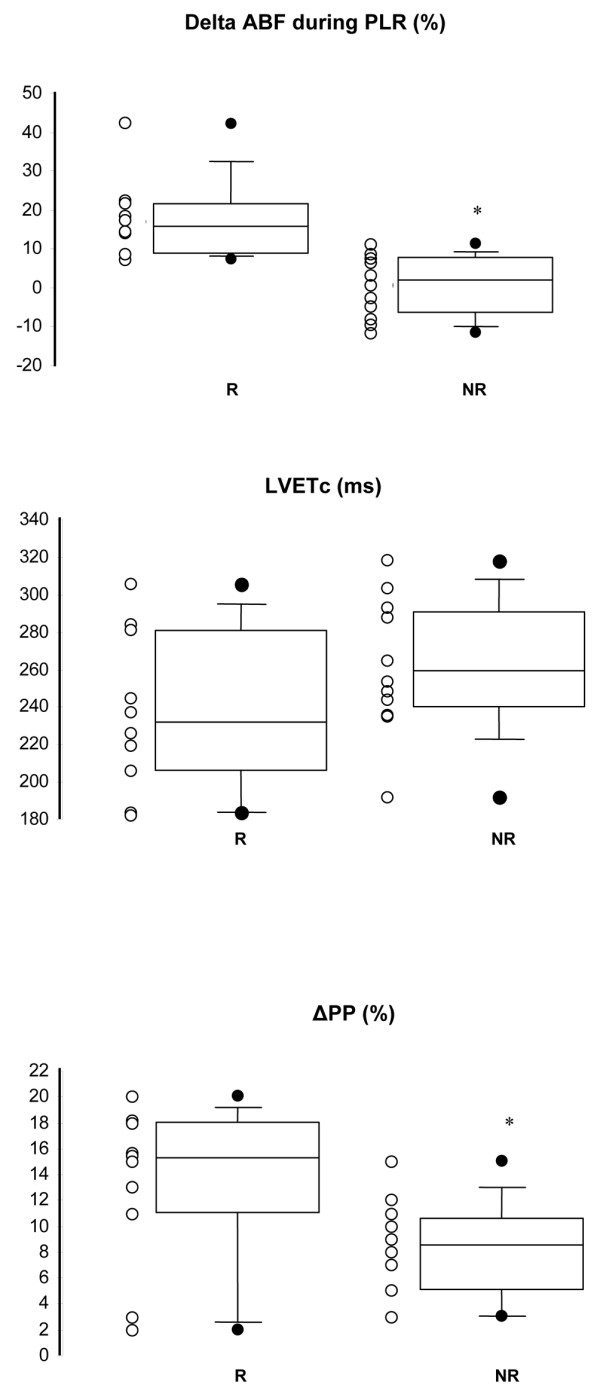
Results: Ten patients were responders and 12 were non-responders. In responders, the increase in ABF induced by PLR was similar to that induced by a 250 ml VE (16% versus 20%; p = 0.15). A PLR-induced increase in ABF of more than 8% predicted fluid responsiveness with a sensitivity of 90% and a specificity of 83%. Corresponding positive and negative predictive values (PPV and NPV, respectively) were 82% and 91%, respectively. A DeltaPP threshold value of 12% predicted fluid responsiveness with a sensitivity of 70% and a specificity of 92%. Corresponding PPV and NPV were 87% and 78%, respectively. A LVETc of 245 ms or less predicted fluid responsiveness with a sensitivity of 70%, and a specificity of 67%. Corresponding PPV and NPV were 60% and 66%, respectively.
Conclusion: The PLR-induced increase in ABF and a DeltaPP of more than 12% offer similar predictive values in predicting fluid responsiveness. An isolated basal LVETc value is not a reliable criterion for predicting response to fluid loading.
Figures

Comment in
-
Can passive leg raising be used to guide fluid administration?Crit Care. 2006;10(6):170. doi: 10.1186/cc5081. Crit Care. 2006. PMID: 17096869 Free PMC article.
References
-
- Valtier B, Cholley BP, Belot JP, de la Coussaye JE, Mateo J, Payen DM. Noninvasive monitoring of cardiac output in critically ill patients using transesophageal Doppler. Am J Respir Crit Care Med. 1998;158:77–83. - PubMed
-
- Singer M, Bennett ED. Noninvasive optimization of left ventricular filling using esophageal Doppler. Crit Care Med. 1991;19:1132–1137. - PubMed
-
- Madan AK, UyBarreta VV, Aliabadi-Wahle S, Jesperson R, Hartz RS, Flint LM, Steinberg SM. Esophageal Doppler ultrasound monitor versus pulmonary artery catheter in the hemodynamic management of critically ill surgical patients. J Trauma. 1999;46:607–611. - PubMed
-
- Michard F, Boussat S, Chemla D, Anguel N, Mercat A, Lecarpentier Y, Richard C, Pinsky MR, Teboul JL. Relation between respiratory changes in arterial pulse pressure and fluid responsiveness in septic patients with acute circulatory failure. Am J Respir Crit Care Med. 2000;162:134–138. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
