

Endovascular treatment of intracranial aneurysms with matrix detachable coils: immediate posttreatment results from a prospective multicenter registry
- PMID: 16971616
- PMCID: PMC8139781
Endovascular treatment of intracranial aneurysms with matrix detachable coils: immediate posttreatment results from a prospective multicenter registry
Abstract
Background and purpose: Endovascular treatment of intracranial aneurysms by using detachable coils has become an accepted alternative to surgery. To reduce the rate of aneurysm recanalization after treatment, biologically active polyglycolic/polylactic acid-covered platinum coils have been proposed. A prospective and multicenter registry was conducted in France to evaluate the safety and short-term and long-term efficacy of Matrix detachable coils. This first analysis is focused on the safety and short-term efficacy.
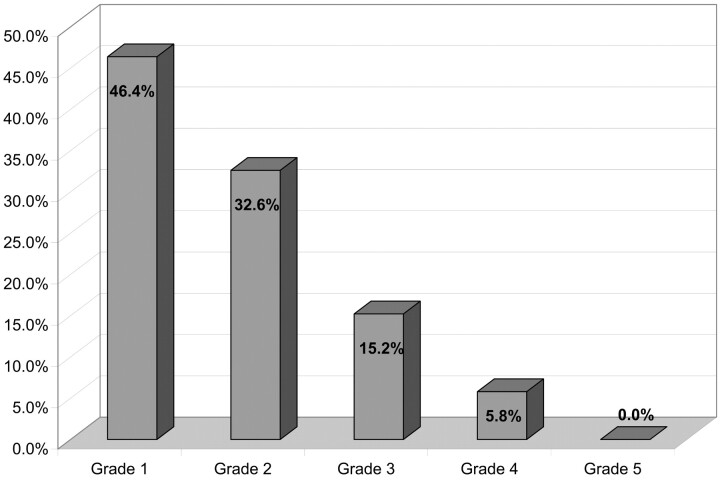
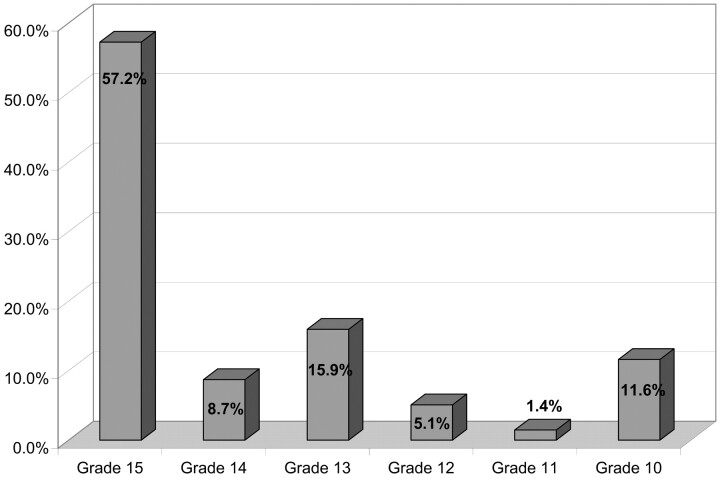
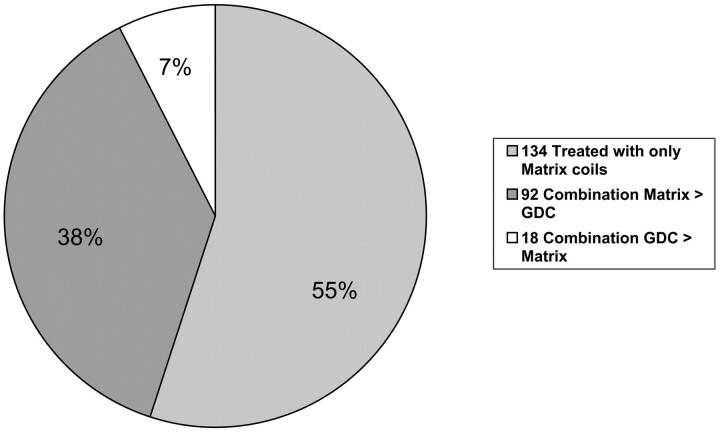
Methods: Two hundred sixty-one patients having ruptured or unruptured aneurysms treated via endovascular approach were included in this registry. Patients with giant aneurysms or in poor clinical condition (Glasgow Coma Scale < 10) were excluded. Because of various protocol violations, clinical analysis was conducted in 236 patients having 244 aneurysms. Technical and clinical complications were systematically recorded. Angiographic analysis was performed by a core laboratory by using the Raymond Grading Scale on 224 patients having 232 aneurysms.
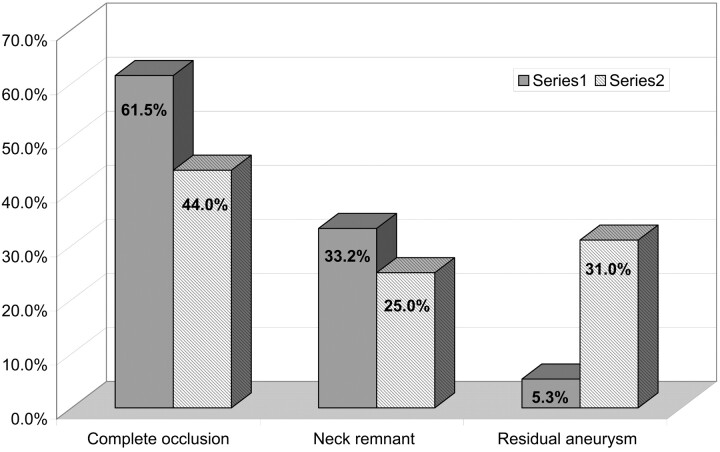
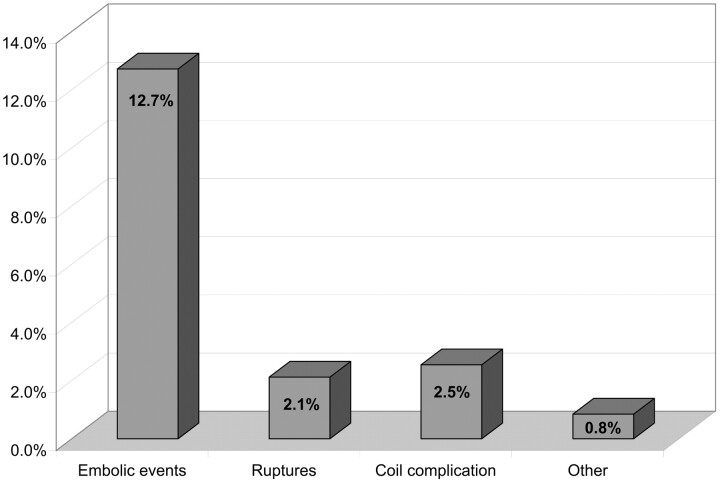
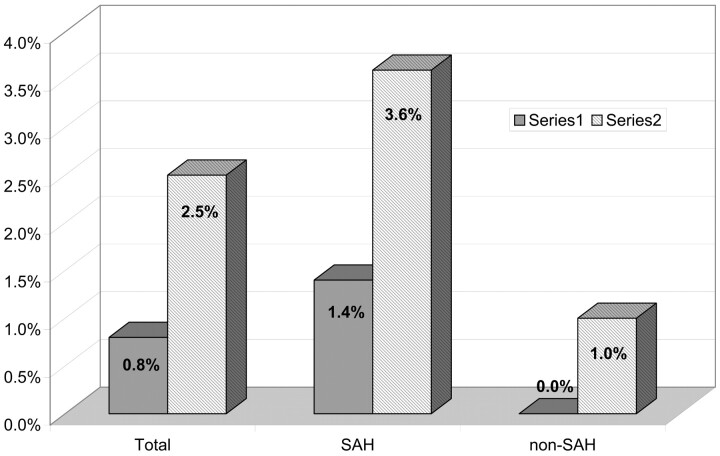
Results: Complete occlusion was achieved in 102 aneurysms (44.0%); neck remnant, in 58 aneurysms (25.0%); and aneurysm remnant, in 72 aneurysms (31.0%). Technical and clinical complications related to the procedure were encountered in 43 patients (18.2%). Postoperative modification of the clinical status was observed in 12 patients (5.1%). Two patients died (0.8%), 6 had a permanent deficit (2.5%), and 4 had a transient deficit (1.7%). Treatment-related mortality was 0.8% and permanent morbidity was 2.5%.
Conclusion: Endovascular treatment of intracranial aneurysms by using Matrix detachable coils is feasible and demonstrated initial angiographic results and overall morbidity and mortality rates that are within the ranges found in the literature in the use of bare platinum coils.
Figures
Comment in
-
Registry on Matrix coils: bias in inclusion, exclusion, and publication.AJNR Am J Neuroradiol. 2007 Mar;28(3):398-9; author reply 399-400. AJNR Am J Neuroradiol. 2007. PMID: 17387810 Free PMC article. No abstract available.
References
-
- Molyneux A, Kerr R, Stratton I, et al; International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet 2002;360:1262–74 - PubMed
-
- Byrne JV, Sohn MJ, Molyneux A. Five-year experience in using coil embolization for ruptured intracranial aneurysm: outcomes and incidence of late rebleeding. J Neurosurg 1999;90:656–63 - PubMed
-
- Cognard C, Weill A, Spelle L, et al. Long-term angiographic follow-up of 169 intracranial berry aneurysms occluded with detachable coils. Radiology 1999;212:348–56 - PubMed
-
- Murayama Y, Nien LN, Duckwiler G, et al. Guglielmi detachable coil embolization of cerebral aneurysms: 11 years’ experience. J Neurosurg 2003;98:959–66 - PubMed
-
- Raymond J, Guilbert F, Weill A, et al. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke 2003;34:1398–403 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical