

Exercise-induced inhibition of angiotensin II vasoconstriction in human thigh muscle
- PMID: 16973706
- PMCID: PMC1890428
- DOI: 10.1113/jphysiol.2006.113977
Exercise-induced inhibition of angiotensin II vasoconstriction in human thigh muscle
Abstract
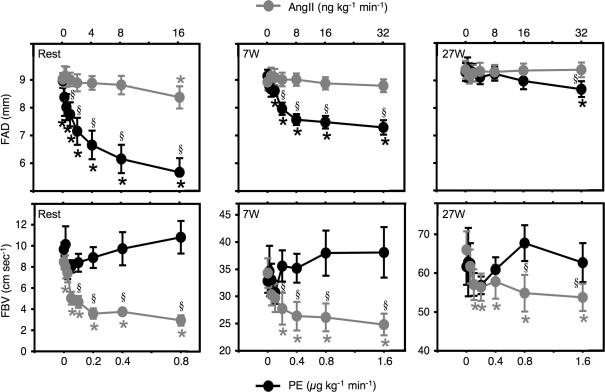
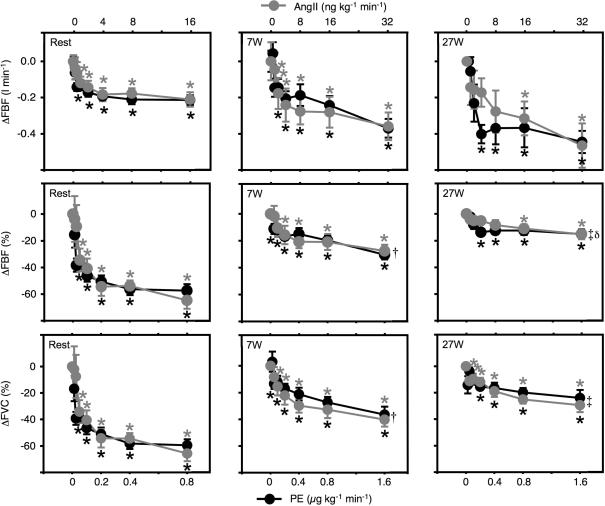
It is well established that metabolic inhibition of adrenergic vasoconstriction contributes to the maintenance of adequate perfusion to exercising skeletal muscle. However, little is known regarding nonadrenergic vasoconstriction during exercise. We tested the hypothesis that a non-adrenergic vasoconstrictor, angiotensin II (AngII), would be less sensitive to metabolic inhibition than an alpha1-agonist, phenylephrine (PE), in the exercising human thigh. In 11 healthy men, femoral blood flow (FBF, ultrasound Doppler and thermodilution) and blood pressure were evaluated during wide-ranging doses of intra-arterial (femoral) infusions of PE and AngII at rest and during two workloads of steady-state knee-extensor exercise (7 W and 27 W). At rest, the maximal decrease in femoral artery diameter (FAD) during AngII (9.0+/-0.2 to 8.4+/-0.4 mm) was markedly less than during PE (9.0+/-0.3 to 5.7+/-0.5 mm), whereas maximal reductions in FBF and femoral vascular conductance (FVC) were similar during AngII (FBF: -65+/-6 and FVC: -66+/-6%) and PE (-57+/-5 and -59+/-4%). During exercise, FAD was not changed by AngII, but moderately decreased by PE. The maximal reductions in FBF and FVC were blunted during exercise compared to rest for both AngII (7 W: -28+/-5 and -40+/-5%; 27 W: -15+/-4% and -29+/-5%) and PE (7 W: -30+/-4 and -37+/-6%; 27 W: -15+/-2 and -24+/-6%), with no significant differences between drugs. The major new findings are (1) an exercise-induced intensity-dependent metabolic attenuation of non-adrenergic vasoconstriction in the human leg; and (2) functional evidence that AngII-vasoconstriction is predominantly distal, whereas alpha1-vasoconstriction is proximal and distal within the muscle vascular bed of the human thigh.
Figures


References
-
- Baan J, Jr, Chang PC, Vermeij P, Pfaffendorf M, Van Zwieten PA. Effects of losartan on vasoconstrictor responses to angiotensin II in the forearm vascular bed of healthy volunteers. Cardiovasc Res. 1996;32:973–979. - PubMed
-
- Blanchet M, Sheppard R, Racine N, Ducharme A, Curnier D, Tardif JC, Sirois P, Lamoureux MC, De Champlain J, White M. Effects of angiotensin-converting enzyme inhibitor plus irbesartan on maximal and submaximal exercise capacity and neurohumoral activation in patients with congestive heart failure. Am J Physiol Heart Circ Physiol. 2005;149:e1–7. - PubMed
-
- Bocqueraz O, Koulmann N, Guigas B, Jimenez C, Melin B. Fluid-regulatory hormone responses during cycling exercise in acute hypobaric hypoxia. Med Sci Sports Exerc. 2004;36:1730–1736. - PubMed
-
- Buckwalter JB, Clifford PS. α-Adrenergic vasoconstriction in active skeletal muscles during dynamic exercise. Am J Physiol Heart Circ Physiol. 1999;277:H33–H39. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical