

Undiagnosed tuberculosis in a community with high HIV prevalence: implications for tuberculosis control
- PMID: 16973982
- PMCID: PMC1899262
- DOI: 10.1164/rccm.200606-759OC
Undiagnosed tuberculosis in a community with high HIV prevalence: implications for tuberculosis control
Abstract
Background: Although failure of tuberculosis (TB) control in sub-Saharan Africa is attributed to the HIV epidemic, it is unclear why the directly observed therapy short-course (DOTS) strategy is insufficient in this setting. We conducted a cross-sectional survey of pulmonary TB (PTB) and HIV infection in a community of 13,000 with high HIV prevalence and high TB notification rate and a well-functioning DOTS TB control program.
Methods: Active case finding for PTB was performed in 762 adults using sputum microscopy and Mycobacterium tuberculosis culture, testing for HIV, and a symptom and risk factor questionnaire. Survey findings were correlated with notification data extracted from the TB treatment register.
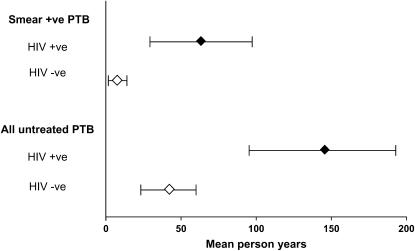
Results: Of those surveyed, 174 (23%) tested HIV positive, 11 (7 HIV positive) were receiving TB therapy, 6 (5 HIV positive) had previously undiagnosed smear-positive PTB, and 6 (4 HIV positive) had smear-negative/culture-positive PTB. Symptoms were not a useful screen for PTB. Among HIV-positive and -negative individuals, prevalence of notified smear-positive PTB was 1,563/100,000 and 352/100,000, undiagnosed smear-positive PTB prevalence was 2,837/100,000 and 175/100,000, and case-finding proportions were 37 and 67%, respectively. Estimated duration of infectiousness was similar for HIV-positive and HIV-negative individuals. However, 87% of total person-years of undiagnosed smear-positive TB in the community were among HIV-infected individuals.
Conclusions: PTB was identified in 9% of HIV-infected individuals, with 5% being previously undiagnosed. Lack of symptoms suggestive of PTB may contribute to low case-finding rates. DOTS strategy based on passive case finding should be supplemented by active case finding targeting HIV-infected individuals.
Figures
Comment in
-
Tuberculosis fueled by HIV: putting out the flames.Am J Respir Crit Care Med. 2007 Jan 1;175(1):6-8. doi: 10.1164/rccm.200609-1376ED. Am J Respir Crit Care Med. 2007. PMID: 17179495 No abstract available.
References
-
- World Health Organization. Global tuberculosis control: surveillance, planning, financing. Geneva, Switzerland: World Health Organization; 2005. WHO Report No. WHO/HTM/TB/2005.349.
-
- World Health Organization. WHO declares TB an emergency in Africa: call for “urgent and extraordinary actions” to halt a worsening epidemic. September 2, 2005. Available from: http://www.who.int/mediacentre/news/africa_emergency/en/ (accessed September 6, 2005).
-
- China Tuberculosis Control Program. Results of directly observed short-course chemotherapy in 112,842 Chinese patients with smear-positive tuberculosis. Lancet 1996;350:169–172. - PubMed
-
- Netto EM, Dye C, Raviglione M. Progress in tuberculosis control 1995–1996, with emphasis on 22 high-income countries. Int J Tuberc Lung Dis 1999;3:310–320. - PubMed
-
- Weis SE, Slocum PC, Blais FX, King B, Nunn M, Matney GB, Gomez E, Foresman BH. The effect of directly observed therapy on the rates of drug resistance and relapses in tuberculosis. N Engl J Med 1994;330:1179–1184. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
