

Accuracy and feasibility of point-of-care and continuous blood glucose analysis in critically ill ICU patients
- PMID: 16981981
- PMCID: PMC1751062
- DOI: 10.1186/cc5048
Accuracy and feasibility of point-of-care and continuous blood glucose analysis in critically ill ICU patients
Abstract
Introduction: To obtain strict glucose regulation, an accurate and feasible bedside glucometry method is essential. We evaluated three different types of point-of-care glucometry in seriously ill intensive care unit (ICU) patients. The study was performed as a single-centre, prospective, observational study in a 12-bed medical ICU of a university hospital.
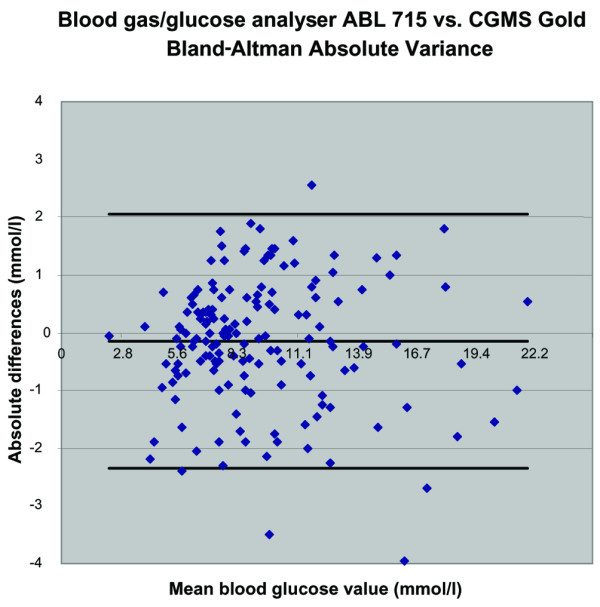
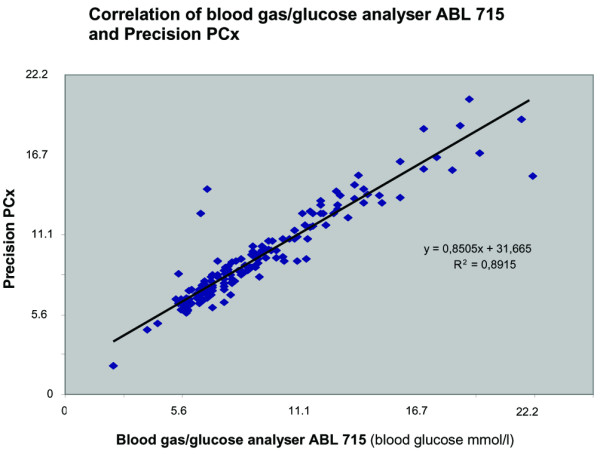
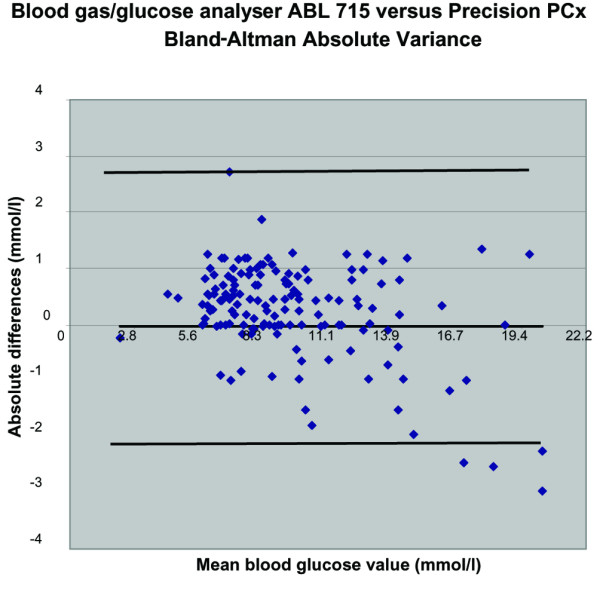
Methods: Patients with an expected ICU stay of more than 48 hours were included. Because the reference laboratory delivers glucose values after approximately 30 to 60 minutes, which is too slow to use in a glucose regulation protocol and for calibration of the subcutaneous continuous glucose monitoring system (CGMS) (CGMS System Gold), we first validated the ICU-based blood gas/glucose analyser ABL715 (part 1 of the study). Subsequently, part 2 was performed: after inserting (and calibrating) the subcutaneous CGMS, heparinised arterial blood samples were drawn from an arterial line every 6 hours and analysed on both the Precision PCx point-of-care meter using test strips and on the blood gas/glucose analyser ABL715. CGMS glucose data were downloaded after 24 to 72 hours. The results of the paired measurements were analysed as a scatter plot by the method of Bland and Altman and were expressed as a correlation coefficient.
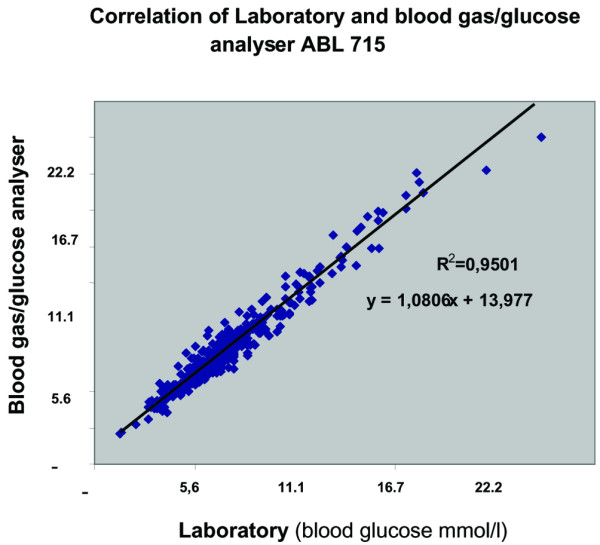
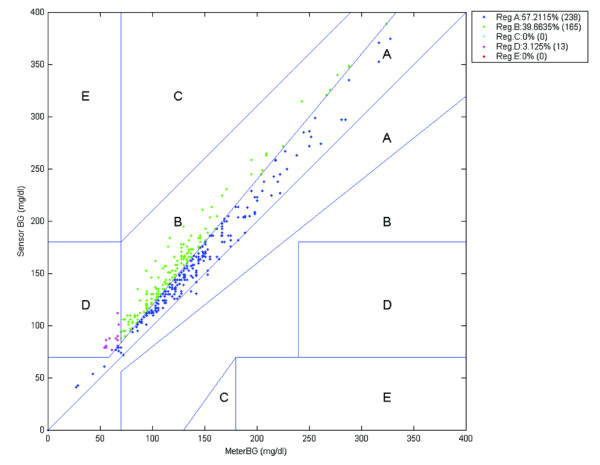
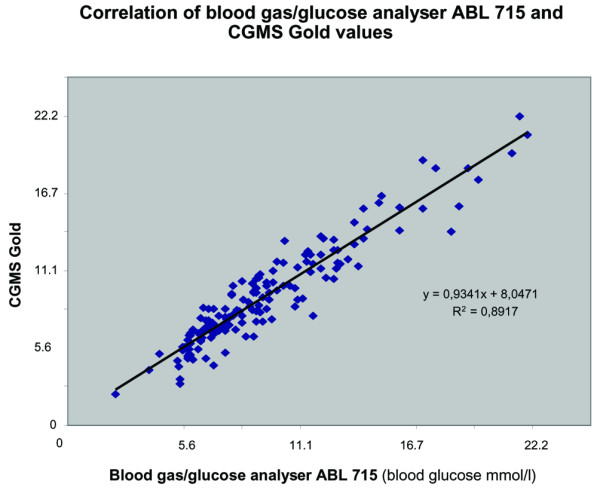
Results: Part 1: Four hundred and twenty-four blood samples were drawn from 45 critically ill ICU patients. The ICU-based blood gas/glucose analyser ABL715 provided a good estimate of conventional laboratory glucose assessment: the correlation coefficient was 0.95. In the Clarke error grid, 96.8% of the paired measurements were in the clinically acceptable zones A and B. Part 2: One hundred sixty-five paired samples were drawn from 19 ICU patients. The Precision PCx point-of-care meter showed a correlation coefficient of 0.89. Ninety-eight point seven percent of measurements were within zones A and B. The correlation coefficient for the subcutaneous CGMS System Gold was 0.89. One hundred percent of measurements were within zones A and B.
Conclusion: The ICU-based blood glucose analyser ABL715 is a rapid and accurate alternative for laboratory glucose determination and can serve as a standard for ICU blood glucose measurements. The Precision PCx is a good alternative, but feasibility may be limited because of the blood sample handling. The subcutaneous CGMS System Gold is promising, but real-time glucose level reporting is necessary before it can be of clinical use in the ICU. When implementing a glucose-insulin algorithm in patient care or research, one should realise that the absolute glucose level may differ systematically among various measuring methods, influencing targeted glucose levels.
Figures
Comment in
-
Blood glucose measurements in the critically ill: more than just a blood draw.Crit Care. 2006;10(6):178. doi: 10.1186/cc5110. Crit Care. 2006. PMID: 17169140 Free PMC article.
References
-
- Krinsley JS. Association between hyperglycemia and increased hospital mortality in a heterogeneous population of critically ill patients. Mayo Clin Proc. 2003;78:1471–1478. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
