

Diagnostic accuracy of preoperative magnetic resonance imaging in predicting curative resection of rectal cancer: prospective observational study
- PMID: 16984925
- PMCID: PMC1602032
- DOI: 10.1136/bmj.38937.646400.55
Diagnostic accuracy of preoperative magnetic resonance imaging in predicting curative resection of rectal cancer: prospective observational study
Abstract
Objective: To assess the accuracy of preoperative staging of rectal cancer with magnetic resonance imaging to predict surgical circumferential resection margins.
Design: Prospective observational study of rectal cancers treated by colorectal multidisciplinary teams between January 2002 and October 2003.
Setting: 11 colorectal units in four European countries.
Participants: 408 consecutive patients presenting with all stages of rectal cancer and undergoing magnetic resonance imaging before total mesorectal excision surgery and histopathological assessment of the surgical specimen.
Main outcome measures: Accuracy of magnetic resonance imaging in predicting a curative resection based on the histological yardstick of presence or absence of tumour at the margins of the specimen.
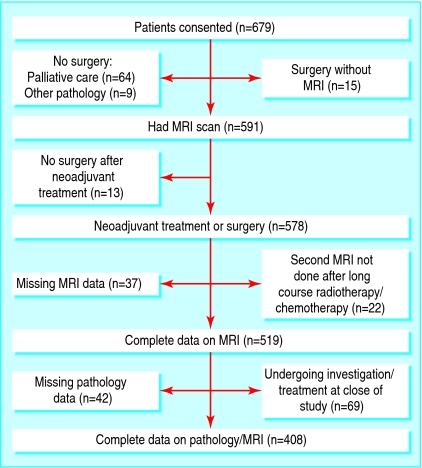
Results: 354 of the 408 patients had a clear circumferential resection margin (87%, 95% confidence interval 83% to 90%). Specificity for prediction of a clear margin by magnetic resonance imaging was 92% (327/354, 90% to 95%). High resolution scans were technically satisfactory in 93% (379/408). Surgical specimens were histopathologically graded as complete or moderate in 80% (328/408), and the median lymph node harvest was 12 (range 0-49). Magnetic resonance imaging predicted clear margins in 349 patients. At surgery 327 had clear margins (94%, 91% to 96%).
Conclusion: High resolution magnetic resonance imaging accurately predicts whether the surgical resection margins will be clear or affected by tumour. This technique can be reproduced accurately in multiple centres to predict curative resection and warns the multidisciplinary team of potential failure of surgery, thus enabling selection of patients for preoperative treatment.
Figures
Comment in
-
Preoperative staging for rectal cancer.BMJ. 2006 Oct 14;333(7572):766-7. doi: 10.1136/bmj.38996.423102.BE. BMJ. 2006. PMID: 17038713 Free PMC article. No abstract available.
-
MRI in predicting curative resection of rectal cancer: defining a "window of opportunity" for laparoscopic surgery.BMJ. 2006 Oct 14;333(7572):808-9. doi: 10.1136/bmj.333.7572.808-b. BMJ. 2006. PMID: 17038744 Free PMC article. No abstract available.
-
MRI in predicting curative resection of rectal cancer: does post-neoadjuvant MRI have a role?BMJ. 2006 Oct 14;333(7572):808. doi: 10.1136/bmj.333.7572.808-a. BMJ. 2006. PMID: 17038745 Free PMC article. No abstract available.
-
Magnetic resonance imaging for rectal cancer.Nat Clin Pract Oncol. 2007 Apr;4(4):222-3. doi: 10.1038/ncponc0767. Epub 2007 Feb 27. Nat Clin Pract Oncol. 2007. PMID: 17325727 No abstract available.
References
-
- Frykholm G, Pahlman L, Glimelius B. Treatment of local recurrences of rectal carcinoma. Radiother Oncol 1995;34: 185-94. - PubMed
-
- Wibe A, Moller B, Norstein J, Carlsen E, Wiig JN, Heald RJ, et al. A national strategic change in treatment policy for rectal cancer—implementation of total mesorectal excision as routine treatment in Norway. A national audit. Dis Colon Rectum 2002;45: 857-66. - PubMed
-
- Martling AL, Holm T, Rutqvist LE, Moran BJ, Heald RJ, Cedemark B. Effect of a surgical training programme on outcome of rectal cancer in the County of Stockholm. Stockholm Colorectal Cancer Study Group, Basingstoke Bowel Cancer Research Project. Lancet 2000;356: 93-6. - PubMed
-
- Sauer R, Becker H, Hohenberger W, Rodel C, Wittekind C, Fietkau R, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 2004;351: 1731-40. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical