

Surveillance strategies for renal cell carcinoma patients following nephrectomy
- PMID: 16985554
- PMCID: PMC1471767
Surveillance strategies for renal cell carcinoma patients following nephrectomy
Abstract
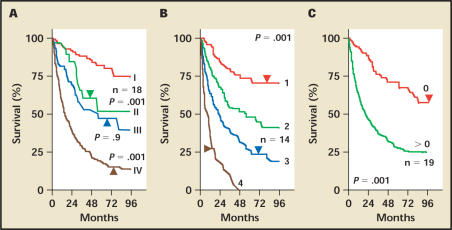
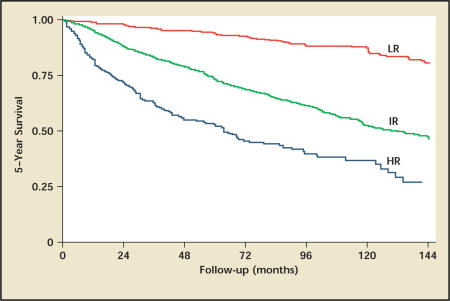
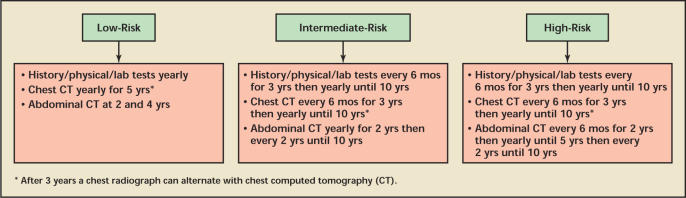
Renal cell carcinoma (RCC) is the most lethal of urologic malignancies, accounting for an estimated 36,000 new cases of carcinoma and 12,000 deaths in 2005. Nephrectomy is the usual treatment; however, after nephrectomy, RCC recurs in 20% to 40% of patients with clinically localized disease. A consensus surveillance protocol does not exist for follow-up of RCC after nephrectomy. In this article, available protocols are reviewed with a goal of developing an evidence-based system including the prognostic factors for recurrent disease, chronology and sites of recurrence, available treatment options if recurrent disease is found, and modalities of diagnostic testing available to urologists. New surveillance recommendations are presented based on prognostic factors as well as the University of California, Los Angeles Integrated Staging System for RCC.
Figures

References
-
- Jemal A, Murray T, Ward E, et al. Cancer statistics, 2005. CA Cancer J Clin. 2005;55:10–30. - PubMed
-
- Janzen NK, Kim HL, Figlin RA, Belldegrun AS. Surveillance after radical or partial nephrectomy for localized renal cell carcinoma and management of recurrent disease. Urol Clin North Am. 2003;30:843–852. - PubMed
-
- Lam JS, Shvarts O, Leppert JT, et al. Renal cell carcinoma 2005: new frontiers in staging, prognostication and targeted molecular therapy. J Urol. 2005;173:1853–1862. - PubMed
-
- Tsui KH, Shvarts O, Smith RB, et al. Prognostic indicators for renal cell carcinoma: a multivariate analysis of 643 patients using the revised 1997 TNM staging criteria. J Urol. 2000;163:1090–1095. quiz 1295. - PubMed
-
- Vasselli JR, Yang JC, Linehan WM, et al. Lack of retroperitoneal lymphadenopathy predicts survival of patients with metastatic renal cell carcinoma. J Urol. 2001;166:68–72. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources