

Benign prostatic hyperplasia: an overview
- PMID: 16985902
- PMCID: PMC1477638
Benign prostatic hyperplasia: an overview
Abstract
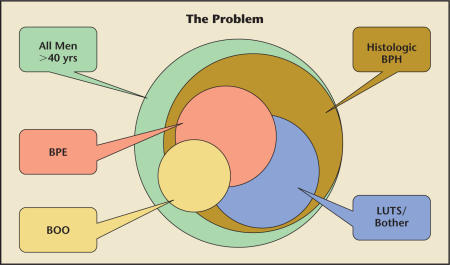
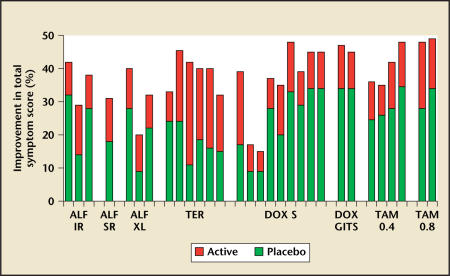
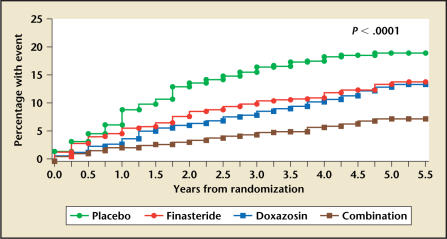
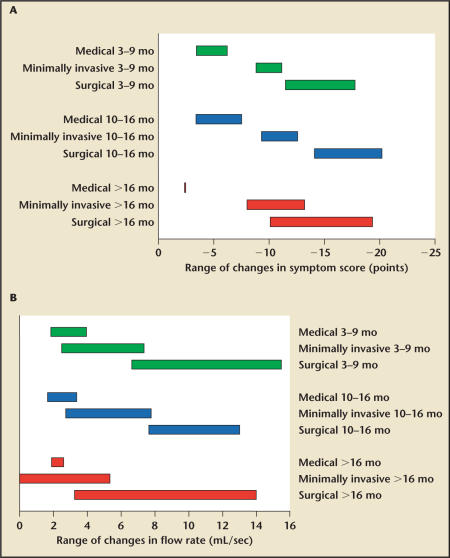
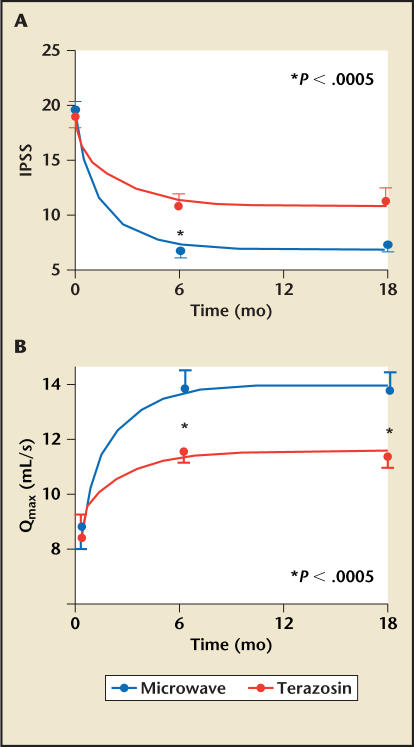
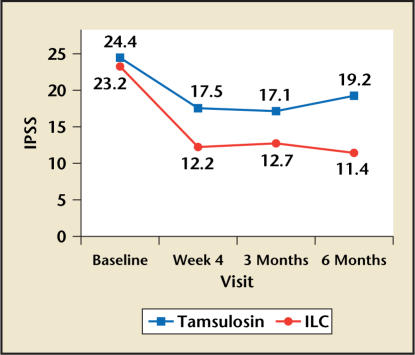
Despite the deceptively simple description of benign prostatic hyperplasia (BPH), the actual relationship between BPH, lower urinary tract symptoms (LUTS), benign prostatic enlargement, and bladder outlet obstruction is complex and requires a solid understanding of the definitional issues involved. The etiology of BPH and LUTS is still poorly understood, but the hormonal hypothesis has many arguments in its favor. There are many medical and minimally invasive treatment options available for affected patients. In the intermediate and long term, minimally invasive treatment options are superior to medical therapy in terms of symptom and flow rate improvement; tissue ablative surgical treatment options are superior to both minimally invasive and medical therapy.
Figures
References
-
- Roehrborn C, McConnell J. Etiology, pathophysiology, epidemiology and natural history of benign prostatic hyperplasia. In: Walsh P, Retik A, Vaughan E, Wein A, editors. Campbell’s Urology. 8th ed. Philadelphia: Saunders; 2002. pp. 1297–1336.
-
- Girman CJ. Population-based studies of the epidemiology of benign prostatic hyperplasia. Br J Urol. 1998;82(suppl 1):34–43. - PubMed
-
- Berry SJ, Coffey DS, Walsh PC, Ewing LL. The development of human benign prostatic hyperplasia with age. J Urol. 1984;132:474–479. - PubMed
-
- Girman CJ, Panser LA, Chute CG, et al. Natural history of prostatism: urinary flow rates in a community-based study. J Urol. 1993;150:887–892. - PubMed
-
- Abrams P. Objective evaluation of bladder outlet obstruction [review] Br J Urol. 1995;76(suppl 1):11–15. - PubMed
LinkOut - more resources
Full Text Sources
Medical