

Hormonal therapy in prostate cancer: historical approaches
- PMID: 16985934
- PMCID: PMC1472891
Hormonal therapy in prostate cancer: historical approaches
Abstract
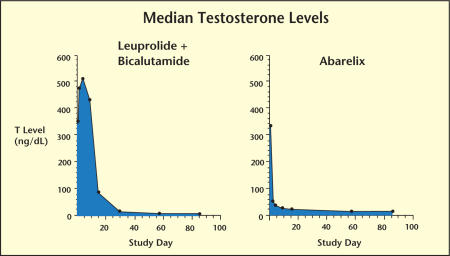
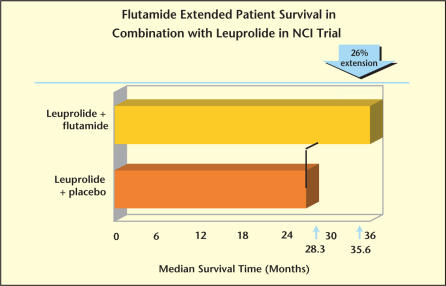
Hormonal therapy has been the standard of care for advanced prostate cancer for over 6 decades. Treatments to suppress testosterone have expanded beyond surgical castration and estrogens to include steroidal and nonsteroidal antiandrogens, luteinizing hormone-releasing hormone agonists, and, most recently, gonadotropin-releasing hormone antagonists. Yet, despite this extensive therapeutic armamentarium, long-term survival of patients with advanced prostate cancer remains poor. Many issues regarding hormonal treatment of prostate cancer continue to be controversial, including the benefits of combined androgen blockade versus monotherapy, the optimal timing of treatment, and the value of new therapeutic approaches and strategies, such as intermittent androgen deprivation and adjuvant chemotherapy.
Figures
References
-
- Huggins C, Hodges CU. Studies on prostate cancer. I. The effect of castration, of estrogen and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer Res. 1941;1:293. - PubMed
-
- Geller J, Albert J, Vik A. Advantages of total androgen blockade in the treatment of advanced prostate cancer. Semin Oncol. 1988;15(suppl 1):53. - PubMed
-
- Huggins C, Scott WW. Bilateral adrenalectomy in prostatic cancer. Ann Surg. 1945;122:1031. - PubMed
-
- Miller GM, Hinman F., Jr Cortisone therapy in advanced carcinoma of the prostate. J Urol. 1954;72:485–496. - PubMed
LinkOut - more resources
Full Text Sources