

Acute urinary retention: risks and management
Abstract
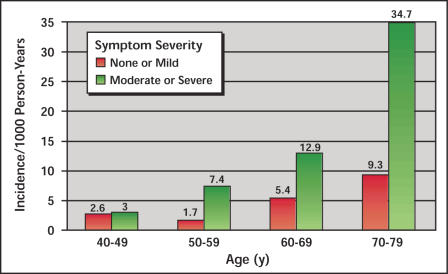
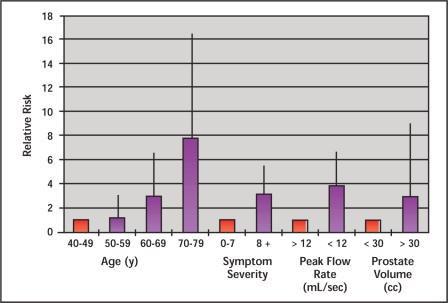
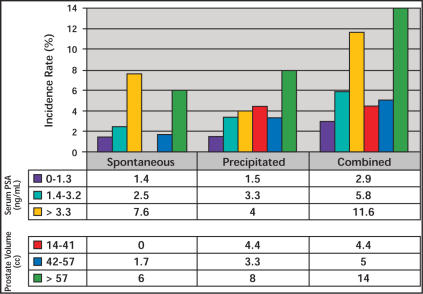
Acute urinary retention (AUR) secondary to benign prostatic hyperplasia has in the past represented an immediate indication for surgery, and today most patients failing to void after an attempt at catheter removal still undergo surgery. The concept that this disease is in fact progressive in nature is slowly being accepted. Descriptive and analytical epidemiological data have shown that the incidence rate per 1000 person-years is less variable in the community than previously assumed; however, the risk is cumulative and increases with advancing age. The risk for patients diagnosed with benign prostatic hyperplasia is naturally higher, and analytical epidemiology has identified several strong risk factors, the most important one being serum prostate-specific antigen (PSA). In addition, prostate volume, maximum flow rate, and symptom severity should be considered when counseling patients presenting with lower urinary tract symptoms and clinical benign prostatic hyperplasia who are considering a course of watchful waiting. Efforts toward primary prevention of AUR should be directed to patients at increased risk, ie, those who are older and have more severe symptoms, larger glands, and higher PSA values. Risk reduction with finasteride has been demonstrated, and alpha-blockers have been shown to aid patients in achieving spontaneous voiding after an episode of AUR.
Figures
References
-
- Holtgrewe HL, Mebust WK, Dowd JB, et al. Transurethral prostatectomies: practical aspects of the dominant operation in American urology. J Urol. 1989;141:248–253. - PubMed
-
- Breum L, Klarskov P, Munck LK, et al. Significance of acute urinary retention due to infravesical obstruction. Scand J Urol Nephrol. 1982;16:21–24. - PubMed
-
- Hastie KJ, Dickinson AJ, Ahmad R, Moisey CU. Acute retention of urine: is trial without catheter justified? J R Coll Surg Edinb. 1990;35:225–227. - PubMed
-
- Klarskov P, Andersen JT, Asmussen CF, et al. Symptoms and signs predictive of the voiding pattern after acute urinary retention in men. Scand J Urol Nephrol. 1987;21:23–28. - PubMed
-
- Powell PH, Smith PJ, Feneley RC. The identification of patients at risk from acute retention. Br J Urol. 1980;52:520–522. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous