

Aromatase inhibitors and bone loss
- PMID: 16986348
- PMCID: PMC2693896
Aromatase inhibitors and bone loss
Abstract
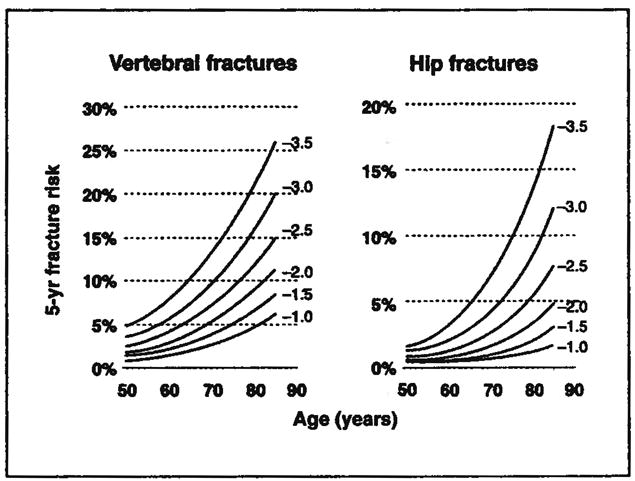
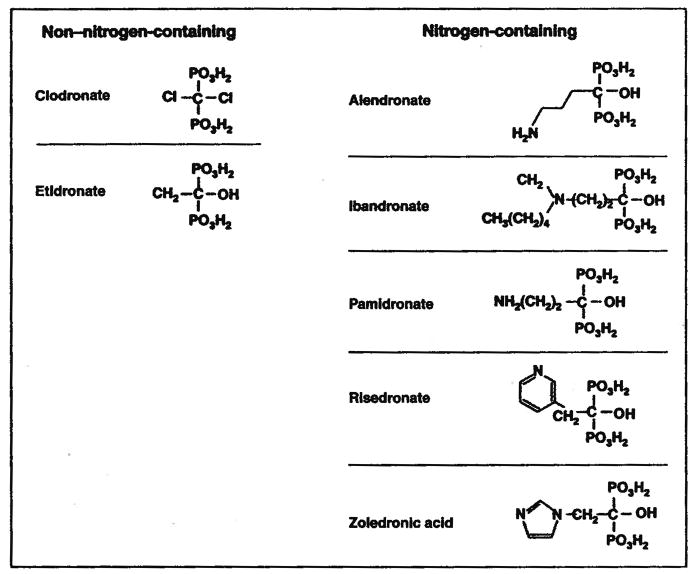
The aromatase inhibitors (AIs) anastrozole (Arimidex), letrozole (Femara), and exemestane (Aromasin) are significantly more effective than the selective estrogen-receptor modulator (SERM) tamoxifen in preventing recurrence in estrogen receptor-positive early breast cancer. Aromatase inhibitors are likely to replace SERMs as first-line adjuvant therapy for many patients. However, AIs are associated with significantly more osteoporotic fractures and greater bone mineral loss. As antiresorptive agents, oral and intravenous bisphosphonates such as alendronate (Fosamax), risedronate (Actonel), ibandronate (Boniva), pamidronate (Aredia), and zoledronic acid (Zometa) have efficacy in preventing postmenopausal osteoporosis, cancer treatment-related bone loss, or skeletal complications of metastatic disease. Clinical practice guidelines recommend baseline and annual follow-up bone density monitoring for all patients initiating AI therapy. Bisphosphonate therapy should be prescribed for patients with osteoporosis (T score < -2.5) and considered on an individual basis for those with osteopenia (T score < -1). Modifiable lifestyle behaviors including adequate calcium and vitamin D intake, weight-bearing exercise, and smoking cessation should be addressed. Adverse events associated with bisphosphonates include gastrointestinal toxicity, renal toxicity, and osteonecrosis of the jaw. These safety concerns should be balanced with the potential of bisphosphonates to minimize or prevent the debilitating effects of AI-associated bone loss in patients with early, hormone receptor-positive breast cancer.
Figures


References
-
- Winer EP, Hudis C, Burstein HJ, et al. American Society of Clinical Oncology technology assessment on the use of aromatase inhibitors as adjuvant therapy for postmenopausal women with hormone receptor–positive breast cancer: Status report 2004. J Clin Oncol. 2005;23:619–629. - PubMed
-
- American Cancer Society. Breast Cancer Facts & Figures 2005–2006. [Accessed July 12, 2006]. Available at www.cancer.org.
-
- Osborne C, Tripathy D. Aromatase inhibitors: Rationale and use in breast cancer. Ann Rev Med. 2005;56:103–116. - PubMed
-
- Mincey BA, Perez EA. Aromatase inhibitors and bone health. ASCO 2005 Education Book; 41st Annual Meeting; Orlando, Florida. 2005. pp. 27–34.
-
- Goss PE, Strasser-Weippl K. Prevention strategies with aromatase inhibitors. Clin Cancer Res. 2004;10(suppl):372s–379s. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
