

Review
doi: 10.3121/cmr.4.3.200.
Postoperative radiotherapy for squamous cell carcinoma of the head and neck
Affiliations
- PMID: 16988100
- PMCID: PMC1570489
- DOI: 10.3121/cmr.4.3.200
Item in Clipboard
Review
Postoperative radiotherapy for squamous cell carcinoma of the head and neck
Clin Med Res.
2006 Sep.
Abstract
This review discusses the role of postoperative radiotherapy (RT) for patients with squamous cell carcinoma of the head and neck. Patients with unfavorable pathologic features have a high-risk of local-regional recurrence and a decreased likelihood of survival after surgery alone. Postoperative RT reduces the risk of local-regional failure and probably improves survival. Patients who are at high risk for recurrence may benefit from more aggressive altered fractionation schedules to decrease the overall time from surgery to the completion of RT. Adjuvant cisplatin-based chemotherapy also appears to improve the probability of cure in high-risk patients.
Figures
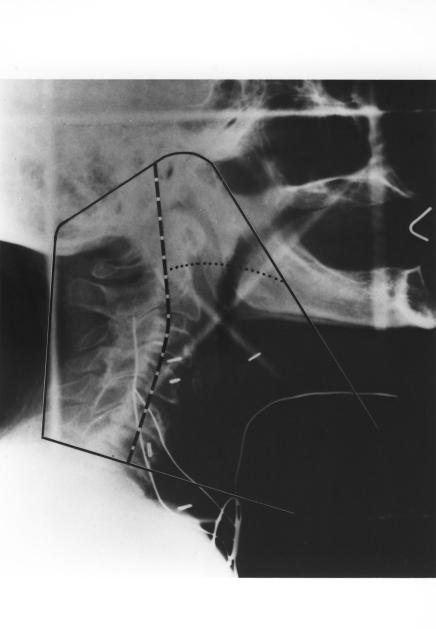
Fields for postoperative irradiation of a patient with advanced cancer of the laryngopharynx. (A) Typical simulation film. The initial “off cord” reduction (50 Gy) is indicated by the dashed line and the final reduction (60 Gy) by the dotted line. Wires mark the surgical scars and stoma. Slanting line used on lower border reduces the length of spinal cord treated by the primary field, allows better caudal coverage of the mucosal surfaces while simultaneously bypassing the shoulders, and facilitates matching the low neck field. (B) Schematic diagram of low neck field. The rectangle (solid line) represents the light field. The dashed lines denote the central axis. The shaded areas represent the blocked portions of the field. The superior border of the neck field is the inferior border of the primary field. The actual line is treated only in the primary field. The upper border of the low neck field assumes a V shape. In the midline of the patient, the apex of the V generally is at or close to the central axis, so that the portion of the low neck portal that treats the spinal cord is nondivergent in its upper portion and diverges away from the primary fields in its lower portion. At the junction of the three fields, a short (2–3 cm) segment of spinal cord remains untreated by any of the three fields (Reprinted with permission of Elsevier from
Amdur RJ et al. Postoperative irradiation for squamous cell carcinoma of the head and neck: an analysis of treatment results and complications. Int J Radiat Oncol Biol Phys
1989;16:25–36.
Copyright 1989 Elsevier. All rights reserved).

Fields for postoperative irradiation of a patient with advanced cancer of the laryngopharynx. (A) Typical simulation film. The initial “off cord” reduction (50 Gy) is indicated by the dashed line and the final reduction (60 Gy) by the dotted line. Wires mark the surgical scars and stoma. Slanting line used on lower border reduces the length of spinal cord treated by the primary field, allows better caudal coverage of the mucosal surfaces while simultaneously bypassing the shoulders, and facilitates matching the low neck field. (B) Schematic diagram of low neck field. The rectangle (solid line) represents the light field. The dashed lines denote the central axis. The shaded areas represent the blocked portions of the field. The superior border of the neck field is the inferior border of the primary field. The actual line is treated only in the primary field. The upper border of the low neck field assumes a V shape. In the midline of the patient, the apex of the V generally is at or close to the central axis, so that the portion of the low neck portal that treats the spinal cord is nondivergent in its upper portion and diverges away from the primary fields in its lower portion. At the junction of the three fields, a short (2–3 cm) segment of spinal cord remains untreated by any of the three fields (Reprinted with permission of Elsevier from
Amdur RJ et al. Postoperative irradiation for squamous cell carcinoma of the head and neck: an analysis of treatment results and complications. Int J Radiat Oncol Biol Phys
1989;16:25–36.
Copyright 1989 Elsevier. All rights reserved).

Typical portal after a hemimandibulectomy, partial maxillectomy and radical neck dissection for a pathologic T4 N0 retromolar trigone lesion. (A) Field reductions were made at 45 Gy (dashed line) and 60 Gy (dotted line). (B) The low neck received 50 Gy given dose (at Dmax) in 25 fractions. The larynx and a segment of the spinal cord were shielded by a tapered midline block (Reprinted with permission of Elsevier from
Amdur RJ et al. Postoperative irradiation for squamous cell carcinoma of the head and neck: an analysis of treatment results and complications. Int J Radiat Oncol Biol Phys
1989;16:25–36.
Copyright 1989 Elsevier. All rights reserved).

Typical portal after a hemimandibulectomy, partial maxillectomy and radical neck dissection for a pathologic T4 N0 retromolar trigone lesion. (A) Field reductions were made at 45 Gy (dashed line) and 60 Gy (dotted line). (B) The low neck received 50 Gy given dose (at Dmax) in 25 fractions. The larynx and a segment of the spinal cord were shielded by a tapered midline block (Reprinted with permission of Elsevier from
Amdur RJ et al. Postoperative irradiation for squamous cell carcinoma of the head and neck: an analysis of treatment results and complications. Int J Radiat Oncol Biol Phys
1989;16:25–36.
Copyright 1989 Elsevier. All rights reserved).
References
-
- American Joint Committee on Cancer. AJCC Cancer Staging Manual. 5th ed. Philadelphia, PA: Lippincott -Raven, 1997. 21–58.
-
- Mendenhall WM, Morris CG, Amdur RJ, Hinerman RW, Mancuso AA. Parameters that predict local control after definitive radiotherapy for squamous cell carcinoma of the head and neck. Head Neck 2003;25:535–542. - PubMed
-
- MacComb WS, Fletcher GH. Planned combination of surgery and radiation in treatment of advanced primary head and neck cancers. Am J Roentgenol Radium Ther Nucl Med 1957;77:397–414. - PubMed
-
- DeSanto LW, Beahrs OH, Holt JJ, O’Fallon WM. Neck dissection and combined therapy. Study of effectiveness. Arch Otolaryngol 1985;111:366–370. - PubMed
-
- Fletcher GH. Basic principles of the combination of irradiation and surgery. Int J Radiat Oncol Biol Phys 1979;5:2091–2096. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical