

An acute care surgery model improves outcomes in patients with appendicitis
- PMID: 16998358
- PMCID: PMC1856575
- DOI: 10.1097/01.sla.0000237756.86181.50
An acute care surgery model improves outcomes in patients with appendicitis
Abstract
Objective: To compare outcomes of appendectomy in an Acute Care Surgery (ACS) model to that of a traditional home-call attending surgeon model.
Summary background data: Acute care surgery (ACS, a combination of trauma surgery, emergency surgery, and surgical critical care) has been proposed as a practice model for the future of general surgery. To date, there are few data regarding outcomes of surgical emergencies in the ACS model.
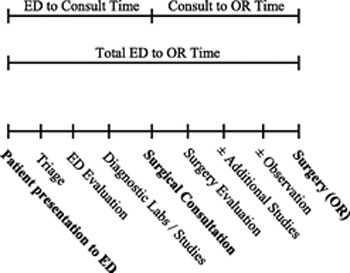
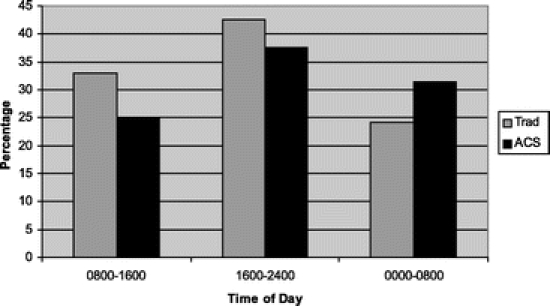
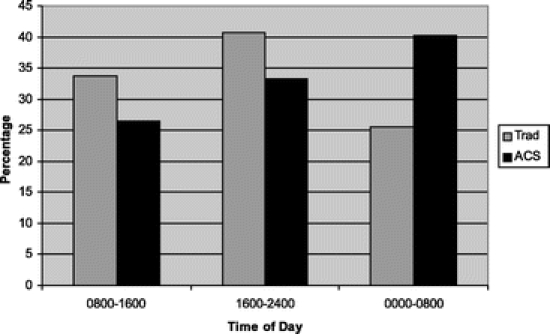
Methods: Between September 1999 and August 2002, surgical emergencies were staffed at the faculty level by either an in-house trauma/emergency surgeon (ACS model) or a non-trauma general surgeon taking home call (traditional [TRAD] model). Coverage alternated monthly. Other aspects of hospital care, including resident complement, remained unchanged. We retrospectively reviewed key time intervals (emergency department [ED] presentation to surgical consultation; surgical consultation to operation [OR]; and ED presentation to OR) and outcomes (rupture rate, negative appendectomy rate, complication rate, and hospital length of stay [LOS]) for patients treated in the ACS and TRAD models. Questions of interest were examined using chi tests for discrete variables and independent sample t test for comparison of means.
Results: During the study period, 294 appendectomies were performed. In-house ACS surgeons performed 167 procedures, and the home-call TRAD surgeons performed 127 procedures. No difference was found in the time from ED presentation to surgical consultation; however, the time interval from consultation to OR was significantly decreased in the ACS model (TRAD 7.6 hours vs. ACS 3.5 hours, P < 0.05). As a result, the total time from ED presentation to OR was significantly shorter in the ACS model (TRAD 14.0 hours vs. ACS 10.1 hour, P < 0.05). Rupture rates were decreased in the ACS model (TRAD 23.3% vs. ACS 12.3%, P < 0.05); negative appendectomy rates were similar. The complication rate in the ACS model was decreased (TRAD 17.4% vs. ACS 7.7%, P < 0.05), as was the hospital LOS (TRAD 3.5 days vs. ACS 2.3 days, P < 0.001).
Conclusions: In patients with acute appendicitis, the presence of an in-house acute care surgeon significantly decreased the time to operation, rupture rate, complication rate, and hospital length of stay. The ACS model appears to improve outcomes of acute appendicitis compared with a TRAD home-call model. This study supports the efficacy and efficiency of the ACS model in the management of surgical emergencies.
Figures
References
-
- Esposito TJ, Leon L, Jurkovich GJ. The shape of things to come: results from a national survey of trauma surgeons on issues concerning their future. J Trauma. 2006;60:8–16. - PubMed
-
- Spain DA, Miller FB. Education and training of the future trauma surgeon in acute care surgery: trauma, critical care, and emergency surgery. Am J Surg. 2005;190:212–217. - PubMed
-
- Kim PK, Dabrowski GP, Reilly PM, et al. Redefining the future of trauma surgery as a comprehensive trauma and emergency general surgery service. J Am Coll Surg. 2004;199:96–101. - PubMed
-
- Asplin BR, Magid DJ, Rhodes KV, et al. A conceptual model of emergency department crowding. Ann Emerg Med. 2003;42:173–180. - PubMed
-
- Derlet RW, Richards JR. Overcrowding in the nation's emergency departments: complex causes and disturbing effects. Ann Emerg Med. 2000;35:63–68. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
