

Hepatic resection for noncolorectal nonendocrine liver metastases: analysis of 1,452 patients and development of a prognostic model
- PMID: 16998361
- PMCID: PMC1856551
- DOI: 10.1097/01.sla.0000239036.46827.5f
Hepatic resection for noncolorectal nonendocrine liver metastases: analysis of 1,452 patients and development of a prognostic model
Abstract
Objective: To determine the utility of hepatic resection (HR) in the treatment of patients with noncolorectal nonendocrine liver metastases (NCNELM).
Summary background data: The place of HR in the treatment of NCNELM remains controversial, primarily due to the limitations of previously published reports and the heterogeneity of primary tumor sites and histologies.
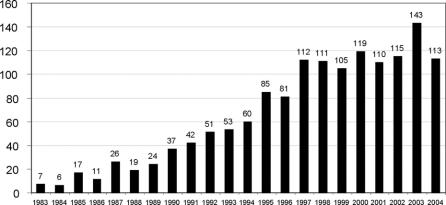
Methods: A multivariate risk model was developed by analyzing prognostic factors and long-term outcomes in 1452 patients with NCNELM treated with HR at 41 centers from 1983 to 2004.
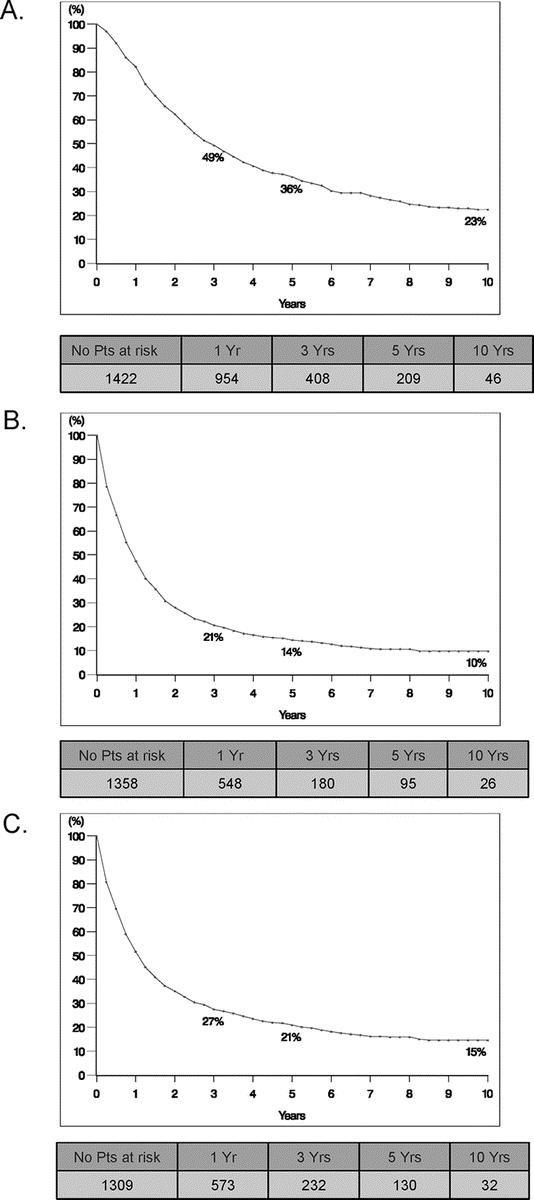
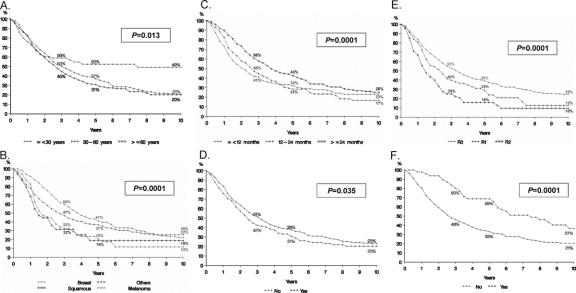
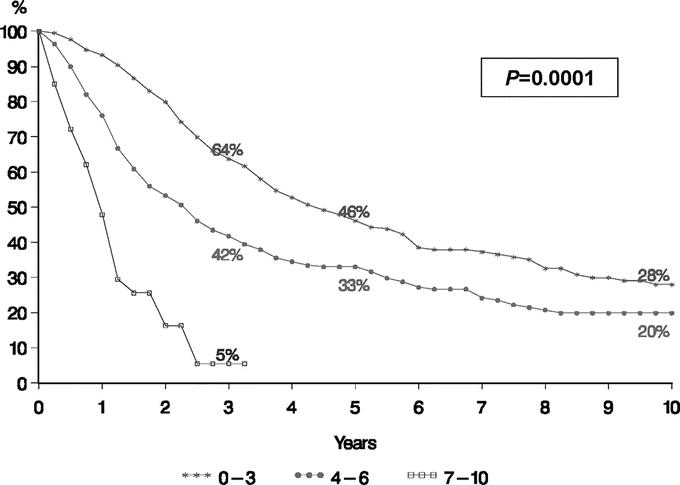
Results: Hepatic metastases were solitary in 56% and unilateral in 71% (mean diameter, 50.5 mm). Extrahepatic metastases were present in 22%. The most common primary sites were breast (32%), gastrointestinal (16%), and urologic (14%). The most common histologies were adenocarcinoma (60%), GIST/sarcoma (13.5%), and melanoma (13%). R0 resection was achieved in 83% of patients with a 60-day mortality rate of 2.3% and a major complication rate of 21.5%. Tumor recurred in 67% of patients (liver, 24%; extrahepatic, 18%; both, 25%). Overall and disease-free survivals at 5 years were 36% and 21% and at 10 years were 23% and 15%, respectively. In multivariate analysis, factors associated with poor prognosis were patient age >60 years, nonbreast origin, melanoma or squamous histology, disease-free interval <12 months, extrahepatic metastases, R2 resection, and major hepatectomy (all P < or = 0.02). A prognostic model based on these factors effectively stratified patients into low-risk (0-3 points, 46% 5-year survival), mid-risk (4-6 points, 33% 5-year survival), and high-risk (>6 points, <10% 5-year survival) groups (P = 0.0001).
Discussion: HR for NCNELM is safe and effective, with outcomes mainly dependent on primary tumor site and histology. For individual patients, a statistical model based on key prognostic factors could validate the indication for hepatic resection by predicting long-term survivals.
Figures
Comment in
-
How safe and effective is hepatic resection for patients with noncolorectal nonendocrine liver metastasis?Nat Clin Pract Gastroenterol Hepatol. 2007 Jun;4(6):310-1. doi: 10.1038/ncpgasthep0818. Epub 2007 May 8. Nat Clin Pract Gastroenterol Hepatol. 2007. PMID: 17489087 No abstract available.
References
-
- Jaeck D, Bachellier P, Guiguet M, et al. Long-term survival following resection of colorectal hepatic metastases: Association Francaise de Chirurgie. Br J Surg. 1997;84:977–980. - PubMed
-
- Scheele J, Stang R, Altendorf-Hofmann A, et al. Resection of colorectal liver metastases. World J Surg. 1995;19:59–71. - PubMed
-
- Stangl R, Altendorf-Hofmann A, et al. Factors influencing the natural history of colorectal liver metastases. Lancet. 1994;343:1405–1410. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
