

A selective approach to the resection of cystic lesions of the pancreas: results from 539 consecutive patients
- PMID: 16998366
- PMCID: PMC1856565
- DOI: 10.1097/01.sla.0000237652.84466.54
A selective approach to the resection of cystic lesions of the pancreas: results from 539 consecutive patients
Abstract
Objective: To define a group of patients with pancreatic cysts who do not require resection.
Summary background data: The increased use of cross-sectional imaging has resulted in an increased identification of small, asymptomatic pancreatic cysts. Data have not been available to determine which lesions should be resected.
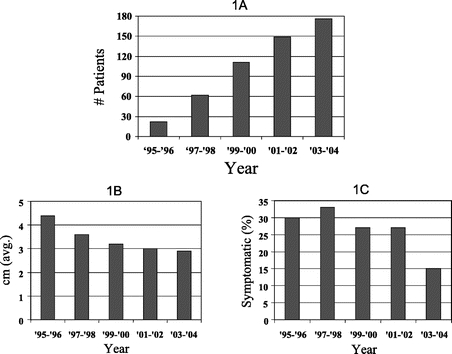
Methods: All patients evaluated at our institution between January 1995 and January 2005 for the ICD-9 diagnosis of pancreatic cyst were reviewed. Analysis was performed to identify associations between patient and cyst characteristics, and selection of operative or nonoperative management.
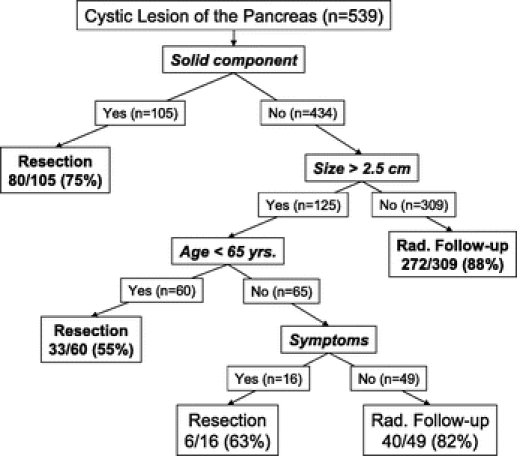
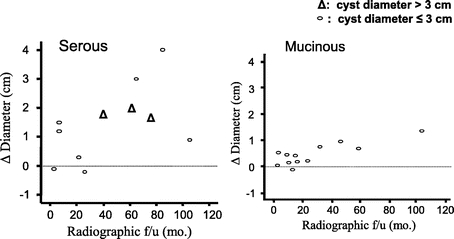
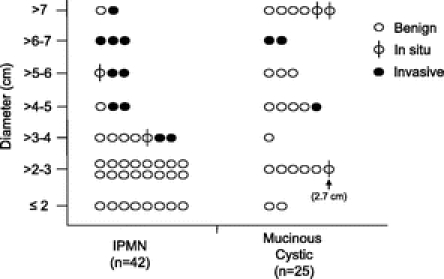
Results: Pancreatic cysts were evaluated in 539 patients. Initial management was operative in 170 patients (32%), and nonoperative (radiographic follow-up) in 369 patients (68%). Factors associated with initial operative management included presence of a solid component (45% vs. 6%, P < 0.001), larger size of the lesion (mean 4.8 cm vs. 2.4 cm, P = 0.001), and presence of symptoms (44% vs. 16%, P = 0.001). Malignancy was present in 18% (32 of 170) of patients initially resected. Mucinous tumors (n = 18) were the most common malignant histologic subtype. None of the invasive cancers arising from mucinous cysts was <3 cm. Median radiographic follow-up in patients initially managed nonoperatively was 24 months (range, 1-172 months). In 29 patients (8%), changes developed within the cyst that resulted in resection; malignancy was present in 11 of 39 (38%), representing 3% (11 of 369) of all patients being followed radiographically.
Conclusions: Selected patients with cystic lesions <3 cm in diameter and without a solid component may be followed radiographically with a malignancy risk (3% this study) that approximates the risk of mortality from resection. Malignancy within mucinous tumors is associated with size, and small mucinous tumors are very unlikely to be malignant.
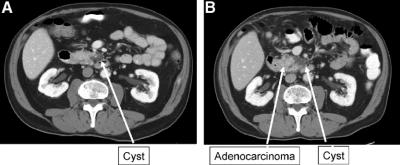
Figures
Comment in
-
A selective approach to resection of cystic lesions of the pancreas: results from 539 consecutive patients.Ann Surg. 2007 May;245(5):825; author reply 825-6. doi: 10.1097/01.sla.0000261097.81200.a8. Ann Surg. 2007. PMID: 17457179 Free PMC article. No abstract available.
-
A selective approach to the resection of cystic lesions of the pancreas: results from 539 consecutive patients.Ann Surg. 2007 May;245(5):826-7; author reply 527-8. doi: 10.1097/01.sla.0000261153.24610.ec. Ann Surg. 2007. PMID: 17457180 Free PMC article. No abstract available.
-
Do all patients with pancreatic cysts need to undergo resection or can some be monitored?Nat Clin Pract Gastroenterol Hepatol. 2007 Jul;4(7):368-9. doi: 10.1038/ncpgasthep0840. Epub 2007 May 15. Nat Clin Pract Gastroenterol Hepatol. 2007. PMID: 17502883 No abstract available.
References
-
- Gorin AD, Sackier JM. Incidental detection of cystic neoplasms of the pancreas. Md Med J. 1997;46:79–82. - PubMed
-
- Brugge WR, Lauwers GY, Sahani D, et al. Cystic neoplasms of the pancreas. N Engl J Med. 2004;351:1218–1226. - PubMed
-
- Sakorafas GH, Sarr MG. Cystic neoplasms of the pancreas: what a clinician should know. Cancer Treat Rev. 2005;31:507–535. - PubMed
-
- Birkmeyer JD, Warshaw AL, Finlayson SR, et al. Relationship between hospital volume and late survival after pancreaticoduodenectomy. Surgery. 1999;126:178–183. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
