

Duodenal switch provides superior weight loss in the super-obese (BMI > or =50 kg/m2) compared with gastric bypass
- PMID: 16998370
- PMCID: PMC1856567
- DOI: 10.1097/01.sla.0000239086.30518.2a
Duodenal switch provides superior weight loss in the super-obese (BMI > or =50 kg/m2) compared with gastric bypass
Abstract
Objectives: Although weight loss following Roux-en-Y gastric bypass is acceptable in patients with preoperative body mass index (BMI) between 35 and 50 kg/m, results from several series demonstrate that failure rates approach 40% when BMI is > or =50 kg/m. Here we report the first large single institution series directly comparing weight-loss outcomes in super-obese patients following biliopancreatic diversion with duodenal switch (DS) and Roux-en-Y Gastric Bypass (RYGB).
Methods: All super-obese patients (BMI > or =50 kg/m) undergoing standardized laparoscopic and open DS and RYGB between August 2002 and October 2005 were identified from a prospective database. Two-sample t tests were used to compare weight loss, decrease in BMI, and percentage of excess body weight loss (% EBWL) after surgery. chi analysis was used to determine the rate of successful weight loss, defined as achieving at least 50% loss of excess body weight.
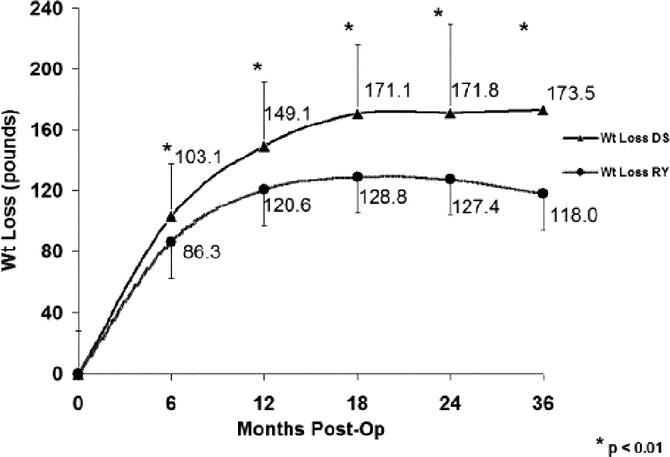
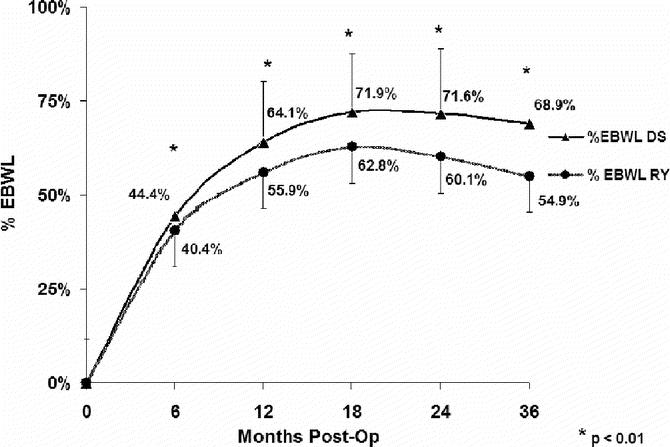
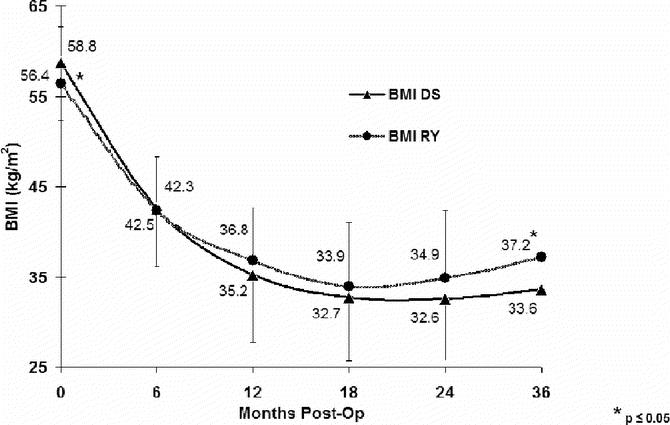
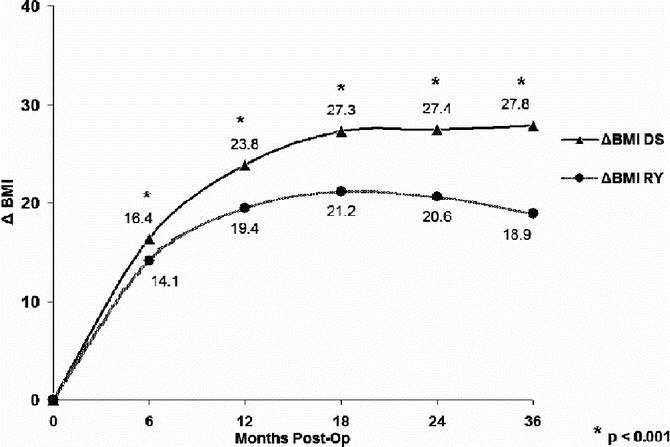
Results: A total of 350 super-obese patients underwent DS (n = 198) or RYGB (n = 152) with equal 30-day mortality (DS,1 of 198; RYGB, 0 of 152; P = not significant). The % EBWL at follow-up was greater for DS than RY (12 months, 64.1% vs. 55.9%; 18 months, 71. 9% vs. 62.8%; 24 months, 71.6% vs. 60.1%; 36 months, 68.9% vs. 54.9%; P < 0.05). Total weight loss and decrease in BMI were also statistically greater for the DS (data not shown). Importantly, the likelihood of successful weight loss (EBWL >50%) was significantly greater in patients following DS (12 months, 83.9% vs. 70.4%; 18 months, 90.3% vs. 75.9%; 36 months, 84.2% vs. 59.3%; P < 0.05).
Conclusions: Direct comparison of DS to RYGB demonstrates superior weight loss outcomes for DS.
Figures
Comment in
-
Is biliopancreatic diversion with duodenal switch the best surgical treatment for super-obese patients?Nat Clin Pract Gastroenterol Hepatol. 2007 May;4(5):250-1. doi: 10.1038/ncpgasthep0791. Nat Clin Pract Gastroenterol Hepatol. 2007. PMID: 17406373 No abstract available.
References
-
- Flegal KM, Carroll MD, Ogden CL, et al. Prevalence and trends in obesity among US adults, 1999–2000. JAMA. 2002;288:1723–1727. - PubMed
-
- Ogden CL, Carroll MD, Curtin LR, et al. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA. 2006;295:1549–1555. - PubMed
-
- Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis: surgical treatment of obesity. Ann Intern Med. 2005;142:547–559. - PubMed
-
- National Institutes of Health Consensus Development Panel. Gastrointestinal surgery for severe obesity. Ann Intern Med. 1991;115:956–961. - PubMed
-
- Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292:1724–1737. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
