

Non-compacted cardiomyopathy: clinical-echocardiographic study
- PMID: 17002802
- PMCID: PMC1592122
- DOI: 10.1186/1476-7120-4-35
Non-compacted cardiomyopathy: clinical-echocardiographic study
Abstract
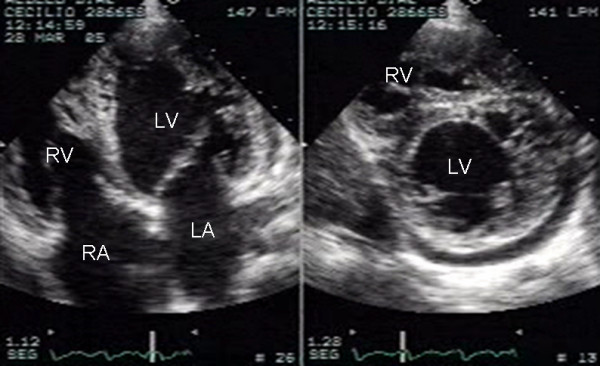
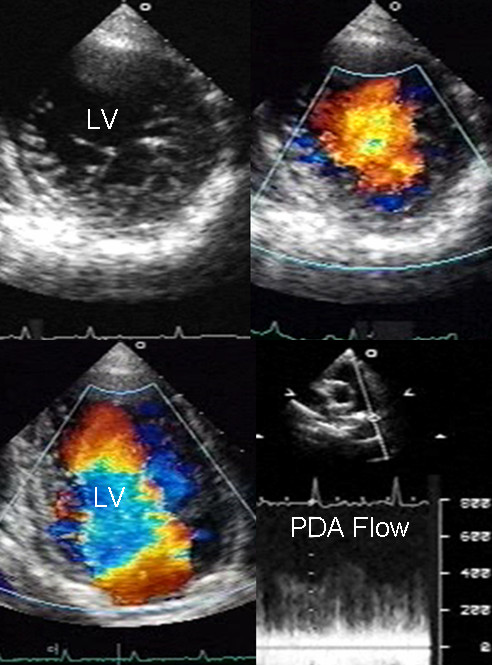
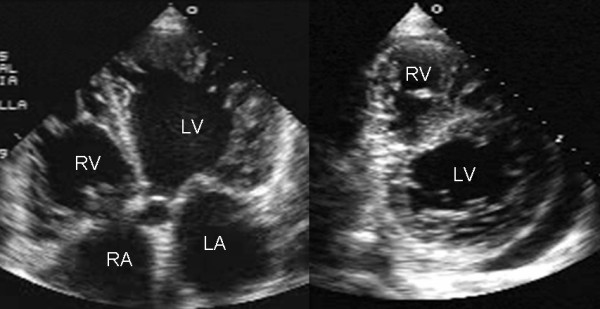
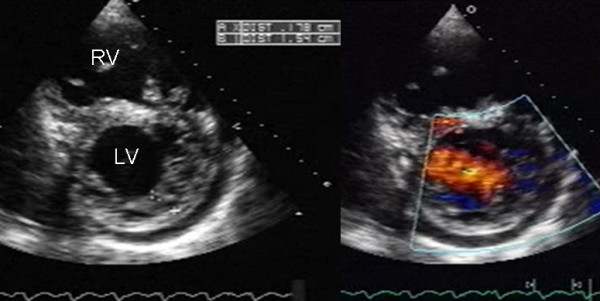
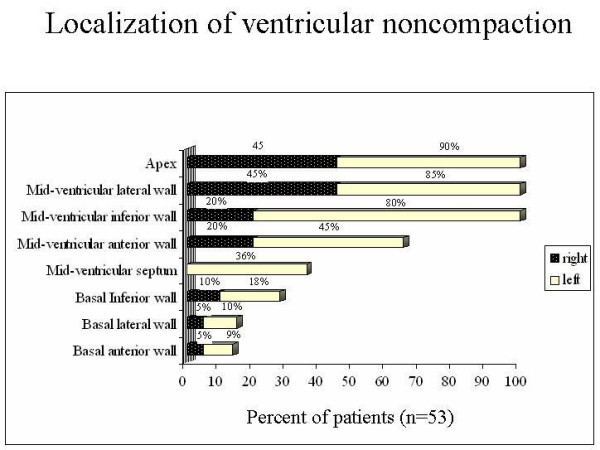
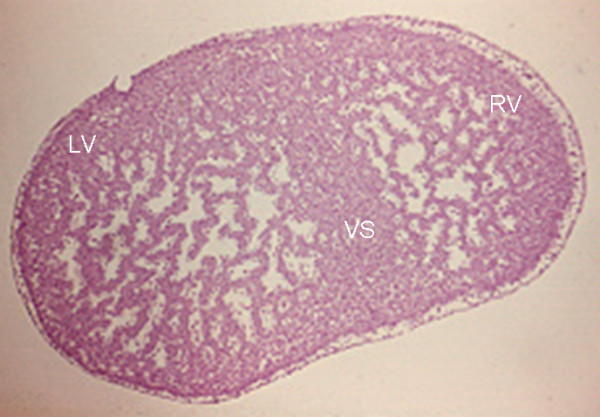
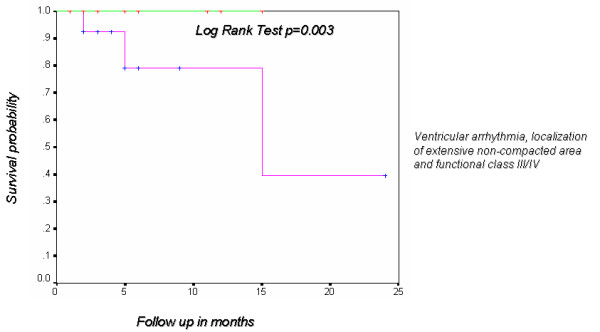
The aim of the present study was to describe the clinical and echocardiographic findings of ventricular noncompaction in adult patients. Fifty-three patients underwent complete clinical history, electrocardiogram, Holter and transthoracic echocardiogram. Forty patients (75%) were in class I/II of the New York Heart Association, and 13 (25%) in class III/IV. Ventricular and supraventricular escape beats were found in 40% and 26.4%, respectively. Holter showed premature ventricular contractions in 32% and sustained ventricular tachycardia in 7.5%. Ventricular noncompaction was an isolated finding in 74% of cases and was associated with other congenital heart disease in 26%. Noncompacted ventricular myocardium involved only left ventricle in 62% of the patients and both ventricles in 38%. The mean ratio of noncompacted to compacted myocardial layers at the site of maximal wall thickness was 3.4 +/- 0.87 mm (range 2.2-7.5). The presence of ventricular noncompaction in more than three segments was associated with a functional class greater than II and ventricular arrhythmia with demonstrable statistical significance by chi2(p < 0.003).
Conclusion: a) Noncompacted cardiomyopathy is a congenital pathological entity that can occur in isolated form or associated with other heart disease and often involves both ventricles. b) A ratio of noncompacted to compacted myocardium greater than 3 and involvement of three or more segments are indicators of poor prognosis. c) Since the clinical manifestations are not sufficient to establish diagnosis, echocardiography is the diagnostic tool that makes it possible to document ventricular noncompaction and establish prognostic factors.
Figures
References
-
- Ritter M, Oechslin E, Sutsch G, Attenhofer C, Schnider J, Jenni R. Isolated noncompaction of the myocardium in adults. Mayo Clin Proc. 1997;72:26–31. - PubMed
-
- Dusek J, Ostadal B, Duskova M. Postnatal persistence of spongy myocardium with embryonic blood supply. Arch Pathol. 1975;99:312–317. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
