

The impact of a decision aid about heart disease prevention on patients' discussions with their doctor and their plans for prevention: a pilot randomized trial
- PMID: 17005051
- PMCID: PMC1626460
- DOI: 10.1186/1472-6963-6-121
The impact of a decision aid about heart disease prevention on patients' discussions with their doctor and their plans for prevention: a pilot randomized trial
Abstract
Background: Low utilization of effective coronary heart disease (CHD) prevention strategies may be due to many factors, but chief among them is the lack of patient involvement in prevention decisions. We undertook this study to test the effectiveness of an individually-tailored, computerized decision aid about CHD on patients' discussions with their doctor and their plans for CHD prevention.
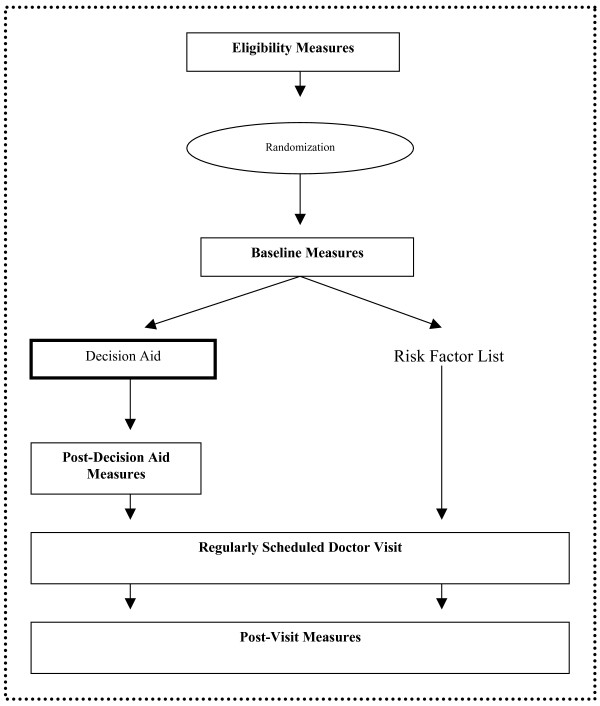
Methods: We conducted a pilot randomized trial in a convenience sample of adults with no previous history of cardiovascular disease to test the effectiveness of an individually-tailored, computerized decision aid about CHD prevention against a risk factor list that patients could present to their doctor.
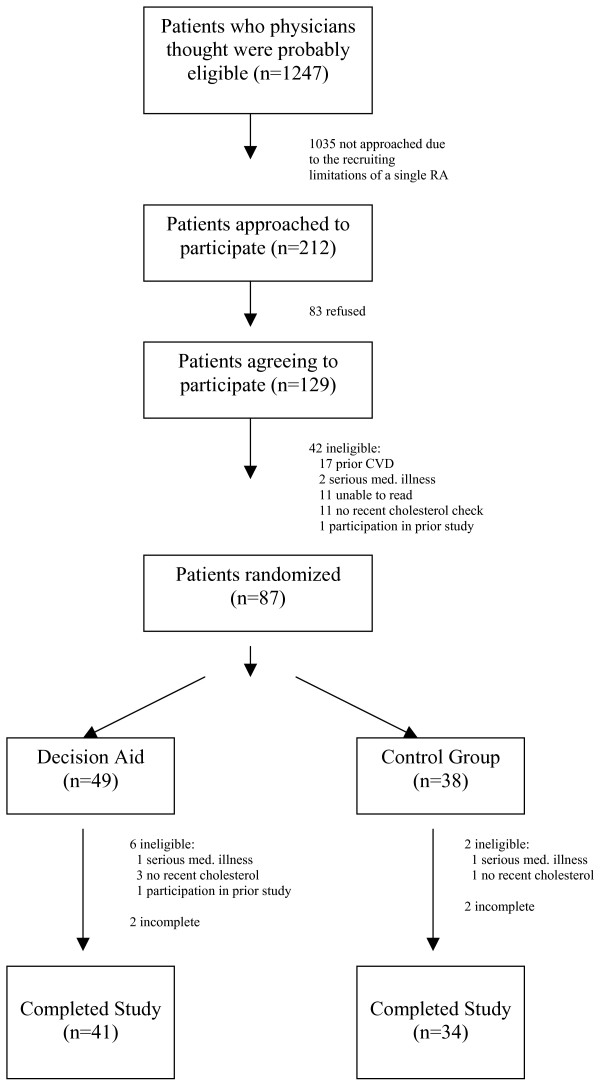
Results: We enrolled 75 adults. Mean age was 53. 59% were female, 73% white, and 23% African-American. 66% had some college education. 43% had a 10-year CHD risk of 0-5%, 25% a risk of 6-10%, 24% a risk of 11-20%, and 5% a risk of > 20%. 78% had at least one option to reduce their CHD risk, but only 45% accurately identified the strategies best supported by evidence. 41 patients received the decision aid, 34 received usual care. In unadjusted analysis, the decision aid increased the proportion of patients who discussed CHD risk reduction with their doctor from 24% to 40% (absolute difference 16%; 95% CI -4% to +37%) and increased the proportion who had a specific plan to reduce their risk from 24% to 37% (absolute difference 13%; 95% CI -7% to +34%). In pre-post testing, the decision aid also appeared to increase the proportion of patients with plans to intervene on their CHD risk (absolute increase ranging from 21% to 47% for planned medication use and 5% to 16% for planned behavioral interventions).
Conclusion: Our study confirms patients' limited knowledge about their CHD risk and effective risk reduction options and provides preliminary evidence that an individually-tailored decision aid about CHD prevention might be expected to increase patients' discussions about CHD prevention with their doctor and their plans for CHD risk reduction. These findings should be replicated in studies with a larger sample size and patients at overall higher risk of CHD.
Trial registration: ClinicalTrials.gov NCT00315978.
Figures
References
-
- Pearson TA, Laurora I, Chu H, Kafonek S. The lipid treatment assessment project (L-TAP): a multicenter survey to evaluate the percentages of dyslipidemic patients receiving lipid- lowering therapy and achieving low-density lipoprotein cholesterol goals. Arch Intern Med. 2000;160:459–67. doi: 10.1001/archinte.160.4.459. - DOI - PubMed
-
- Folsom AR, Sprafka JM, Luepker RV, Jacobs DR., Jr Beliefs among black and white adults about causes and prevention of cardiovascular disease: the Minnesota Heart Survey. Am J Prev Med. 1988;4:121–7. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
