

Can anesthetic technique for primary breast cancer surgery affect recurrence or metastasis?
- PMID: 17006061
- PMCID: PMC1615712
- DOI: 10.1097/00000542-200610000-00008
Can anesthetic technique for primary breast cancer surgery affect recurrence or metastasis?
Abstract
Background: Regional anesthesia is known to prevent or attenuate the surgical stress response; therefore, inhibiting surgical stress by paravertebral anesthesia might attenuate perioperative factors that enhance tumor growth and spread. The authors hypothesized that breast cancer patients undergoing surgery with paravertebral anesthesia and analgesia combined with general anesthesia have a lower incidence of cancer recurrence or metastases than patients undergoing surgery with general anesthesia and patient-controlled morphine analgesia.
Methods: In this retrospective study, the authors examined the medical records of 129 consecutive patients undergoing mastectomy and axillary clearance for breast cancer between September 2001 and December 2002.
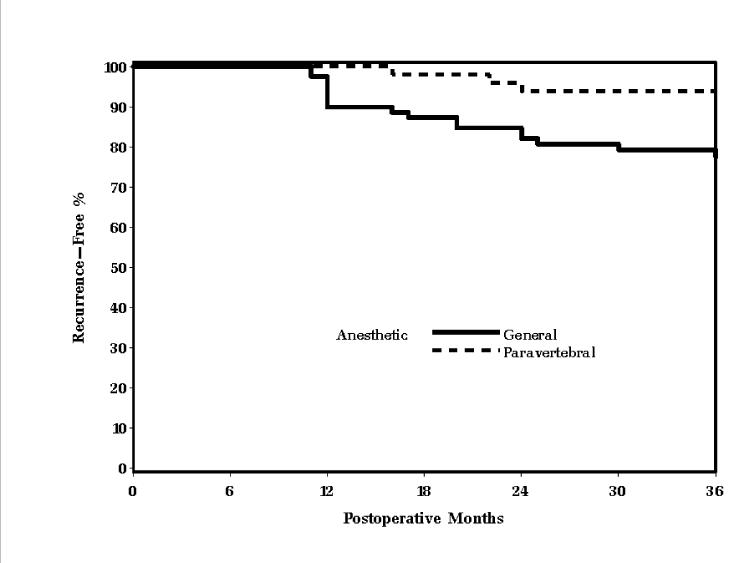
Results: Fifty patients had surgery with paravertebral anesthesia and analgesia combined with general anesthesia, and 79 patients had general anesthesia combined with postoperative morphine analgesia. The follow-up time was 32 +/- 5 months (mean +/- SD). There were no significant differences in patients or surgical details, tumor presentation, or prognostic factors. Recurrence- and metastasis-free survival was 94% (95% confidence interval, 87-100%) and 82% (74-91%) at 24 months and 94% (87-100%) and 77% (68-87%) at 36 months in the paravertebral and general anesthesia patients, respectively (P = 0.012).
Conclusions: This retrospective analysis suggests that paravertebral anesthesia and analgesia for breast cancer surgery reduces the risk of recurrence or metastasis during the initial years of follow-up. Prospective trials evaluating the effects of regional analgesia and morphine sparing on cancer recurrence seem warranted.
Figures
Comment in
-
Retrospective analysis: looking backward to point the way forward.Anesthesiology. 2006 Oct;105(4):643-4. doi: 10.1097/00000542-200610000-00003. Anesthesiology. 2006. PMID: 17006057 No abstract available.
-
Regional block and cancer recurrence: too early to tell.Anesthesiology. 2007 Aug;107(2):354; author reply 354-5. doi: 10.1097/01.anes.0000271919.18782.f4. Anesthesiology. 2007. PMID: 17667583 No abstract available.
-
Paravertebral anesthesia: how substance P and the NK-1 receptor could be involved in regional block and breast cancer recurrence.Breast Cancer Res Treat. 2010 Jul;122(2):601-3. doi: 10.1007/s10549-010-0850-y. Epub 2010 Mar 24. Breast Cancer Res Treat. 2010. PMID: 20333544 No abstract available.
-
Perioperative fluid management: science, art or random chaos?Br J Anaesth. 2015 May;114(5):717-21. doi: 10.1093/bja/aev067. Epub 2015 Mar 19. Br J Anaesth. 2015. PMID: 25794505 No abstract available.
References
-
- Dixon M. ABC of Breast Diseases. 2nd Edition Vol. 4. BMJ Publishing; London: 2000. pp. 75–80.
-
- Ben-Eliyahu S. The price of anticancer intervention. Does surgery promote metastasis? Lancet Oncol. 2002;3:578–9. - PubMed
-
- Kehlet H. Modification of responses to surgery by neural blockade: clinical implications In: Neural blockade in clinical anesthesia and pain management. In: Cousins M, Bridenbough M, editors. Vol. 5. Lippincott-Raven; Philadelphia: 1998. pp. 129–75.
-
- Karmakar MK. Thoracic paravertebral block. Anesthesiology. 2001;95:771–80. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
