

Review
doi: 10.3748/wjg.v12.i35.5611.
Upper gastrointestinal function and glycemic control in diabetes mellitus
Affiliations
- PMID: 17007012
- PMCID: PMC4088160
- DOI: 10.3748/wjg.v12.i35.5611
Item in Clipboard
Review
Upper gastrointestinal function and glycemic control in diabetes mellitus
World J Gastroenterol.
.
Abstract
Recent evidence has highlighted the impact of glycemic control on the incidence and progression of diabetic micro- and macrovascular complications, and on cardiovascular risk in the non-diabetic population. Postprandial blood glucose concentrations make a major contribution to overall glycemic control, and are determined in part by upper gastrointestinal function. Conversely, poor glycemic control has an acute, reversible effect on gastrointestinal motility. Insights into the mechanisms by which the gut contributes to glycemia have given rise to a number of novel dietary and pharmacological strategies designed to lower postprandial blood glucose concentrations.
Figures
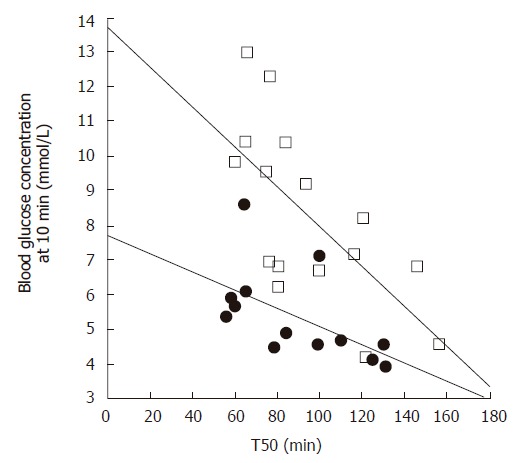
Relationship between the blood glucose concentration 10 min after consuming 75 g glucose in 300 mL water, and the gastric half-emptying time (T50) in patients with type 2 diabetes (open squares, r = -0.67, P < 0.005) and healthy subjects (filled circles, r = -0.56, P < 0.05). Adapted from Jones et al 1996[28].
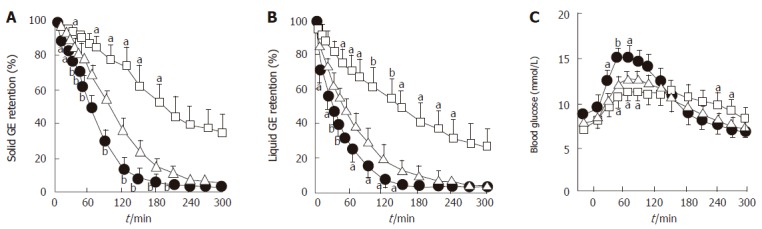
Effects of erythromycin (200 mg iv, filled circles) and morphine (8 mg iv, open squares) compared to placebo (open triangles) on (A) solid and (B) liquid gastric emptying and (C) blood glucose concentration in 9 patients with type 2 diabetes. aP < 0.05, bP < 0.01 vs placebo. Adapted from Gonlachanvit et al 2003[29].
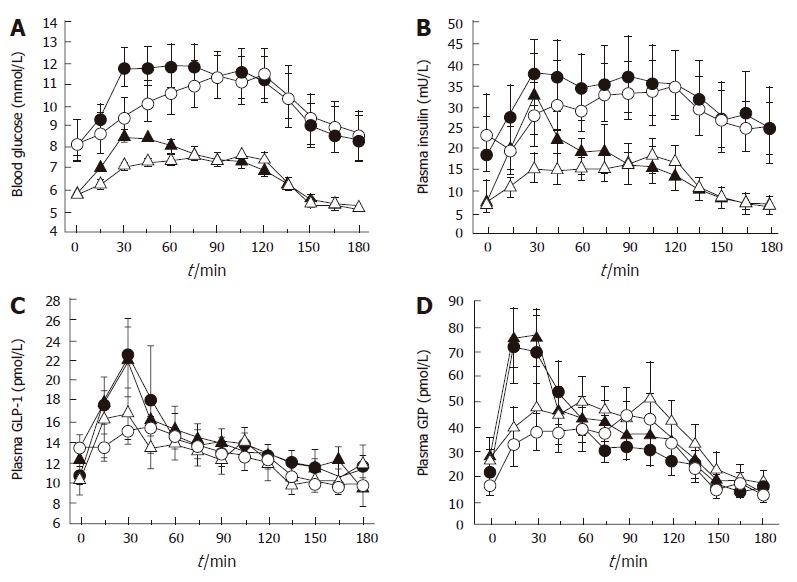
Effect of initially more rapid intraduodenal glucose infusion (3 kcal/min between t = 0 and 15 min and 0.71 kcal/min between t = 15 and 120 min) (closed symbols) compared to constant infusion (1 kcal/min between t = 0 and 120 min) (open symbols) in healthy subjects (triangles) and patients with type 2 diabetes (circles) on (A) blood glucose, (B) plasma insulin, (C) plasma GLP-1, and (D) plasma GIP. Each pair of curves differs between 0 and 30 min for variable vs constant intraduodenal infusion (P < 0.05). Adapted from O’Donovan et al 2004[52].
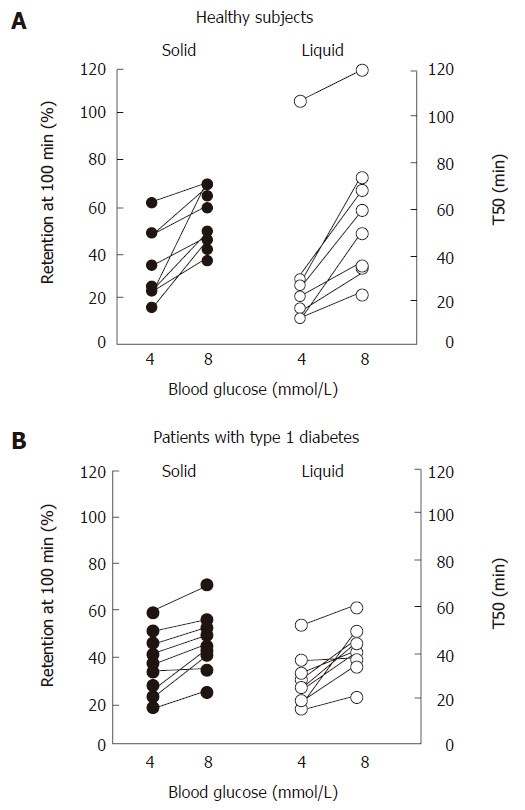
Solid and liquid gastric emptying in (A) healthy subjects and (B) patients with type 1 diabetes mellitus during euglycemia (blood glucose 4 mmol/L) and “physiological” hyperglycemia (blood glucose 8 mmol/L). Adapted from Schvarcz et al 1997[82].
References
-
- Mokdad AH, Ford ES, Bowman BA, Nelson DE, Engelgau MM, Vinicor F, Marks JS. Diabetes trends in the U.S.: 1990-1998. Diabetes Care. 2000;23:1278–1283. - PubMed
-
- Prevalence of diabetes and impaired fasting glucose in adults--United States, 1999-2000. MMWR Morb Mortal Wkly Rep. 2003;52:833–837. - PubMed
-
- Dunstan DW, Zimmet PZ, Welborn TA, De Courten MP, Cameron AJ, Sicree RA, Dwyer T, Colagiuri S, Jolley D, Knuiman M, et al. The rising prevalence of diabetes and impaired glucose tolerance: the Australian Diabetes, Obesity and Lifestyle Study. Diabetes Care. 2002;25:829–834. - PubMed
-
- Del Prato S. In search of normoglycaemia in diabetes: controlling postprandial glucose. Int J Obes Relat Metab Disord. 2002;26 Suppl 3:S9–17. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
