

Preoperative estimation of residual volume for WHO grade II glioma resected with intraoperative functional mapping
- PMID: 17018698
- PMCID: PMC1828101
- DOI: 10.1215/15228517-2006-015
Preoperative estimation of residual volume for WHO grade II glioma resected with intraoperative functional mapping
Abstract
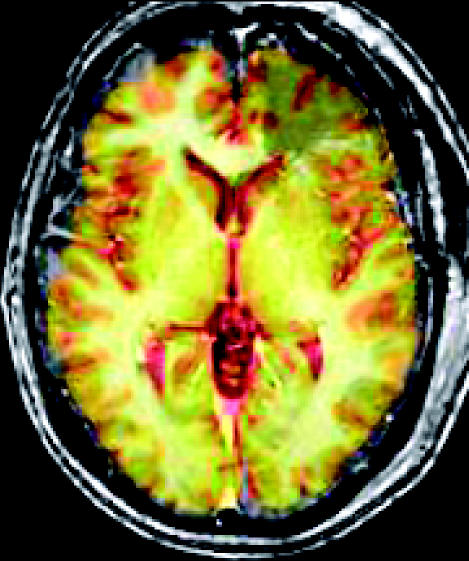
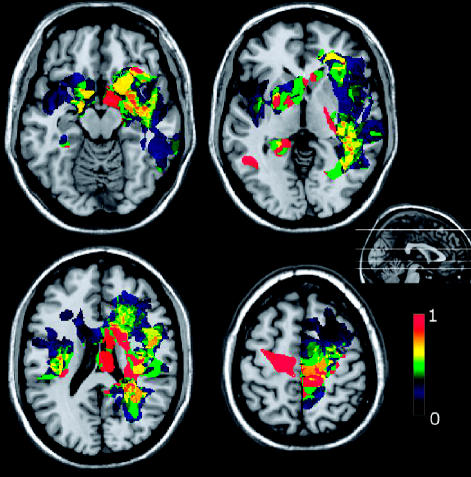
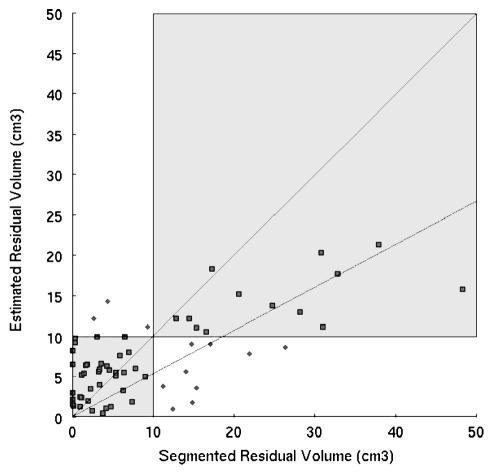
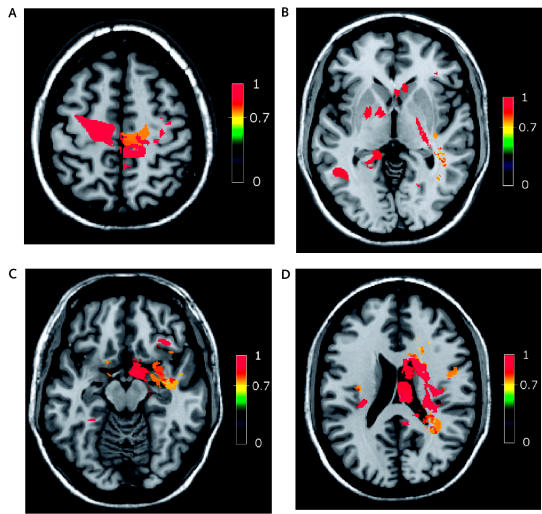
Despite the lack of class I evidence, it is widely agreed that surgery can improve the functional and vital prognosis for WHO grade II gliomas when the resection is at least subtotal radiologically, that is, leaving less than 10 cm(3) of visible residual tumor. Because these tumors frequently invade functional areas, the preoperative estimation of the probable residual volume remains challenging. This article presents a probabilistic map of postoperative residues, with the aim of predicting before the decision for surgical intervention whether the resection could be subtotal. We selected 65 patients who underwent surgery with intraoperative functional mapping between 1999 and 2004 for a WHO grade II glioma located in a sensorimotor and/or language area. For each case, the postoperative image was normalized on a standard atlas, and the residual tumor was segmented. A probabilistic map of residues was then computed. The fusion between the map and a preoperative image allowed a preoperative estimation of the expected extent of resection. The map enhances the regions where grade II glioma cannot be resected. The success rate for the preoperative classification of partial versus subtotal resection is 82%. Although both its reliability and accuracy have to be improved, this probabilistic map gives preoperatively an objective estimation of the expected extent of resection for grade II glioma resected under intraoperative functional mapping. This rationale will assist in decisions regarding surgical resection and may thus contribute to the elaboration of a therapeutic consensus for WHO grade II glioma.
Figures
References
-
- Ashby LS, Shapiro WR. Low-grade glioma: Supratentorial astrocytoma, oligodendroglioma, and oligoastrocytoma in adults. Curr Neurol Neurosci Rep. 2004;4:211–217. - PubMed
-
- Aubert A, Costalat R, Duffau H, Benali H. Modeling of pathophysiological coupling between brain electrical activation, energy metabolism and hemodynamics: Insights for the interpretation of intra-cerebral tumor imaging. Acta Biotheor. 2002;50:281–295. - PubMed
-
- Berger MS, Deliganis AV, Dobbins J, Keles GE. The effect of extent of resection on recurrence in patients with low grade cerebral hemisphere gliomas. Cancer. 1994;74:1784–1791. - PubMed
-
- Brett M, Leff AP, Rorden C, Ashburner J. Spatial normalization of brain images with focal lesions using cost function masking. Neuroimage. 2001;14:486–500. - PubMed
-
- Brett M, Johnsrude IS, Owen AM. The problem of functional localization in the human brain. Nat Rev Neurosci. 2002;3:243–249. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
