

A comparative analysis of influenza vaccination programs
- PMID: 17020406
- PMCID: PMC1584413
- DOI: 10.1371/journal.pmed.0030387
A comparative analysis of influenza vaccination programs
Abstract
Background: The threat of avian influenza and the 2004-2005 influenza vaccine supply shortage in the United States have sparked a debate about optimal vaccination strategies to reduce the burden of morbidity and mortality caused by the influenza virus.
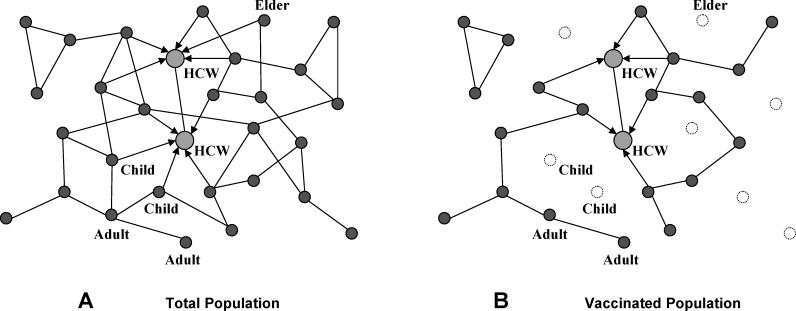
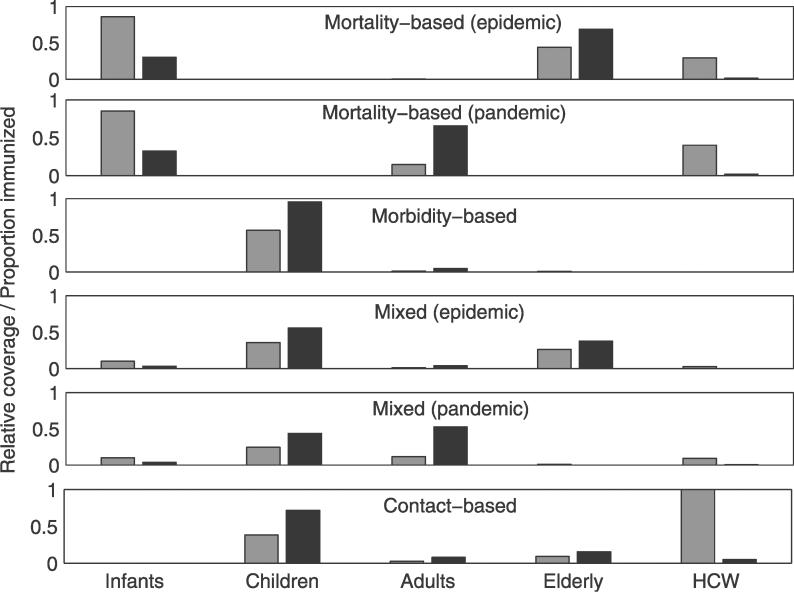
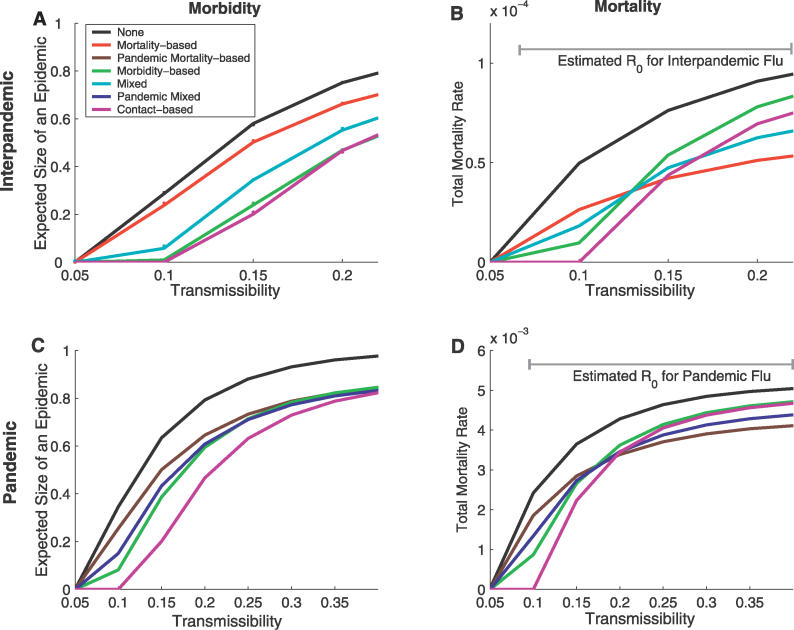
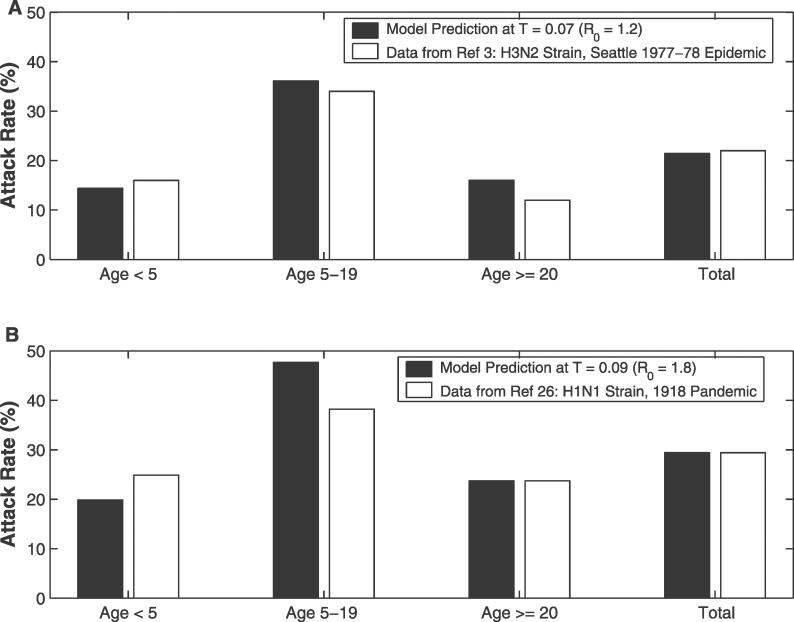
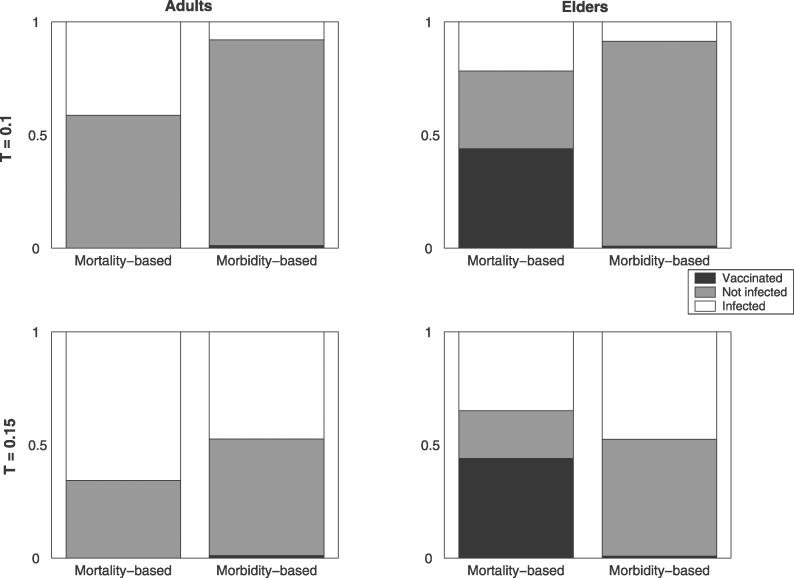
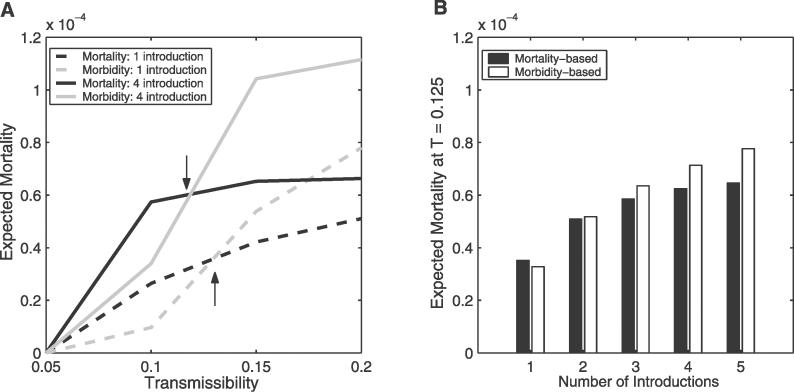
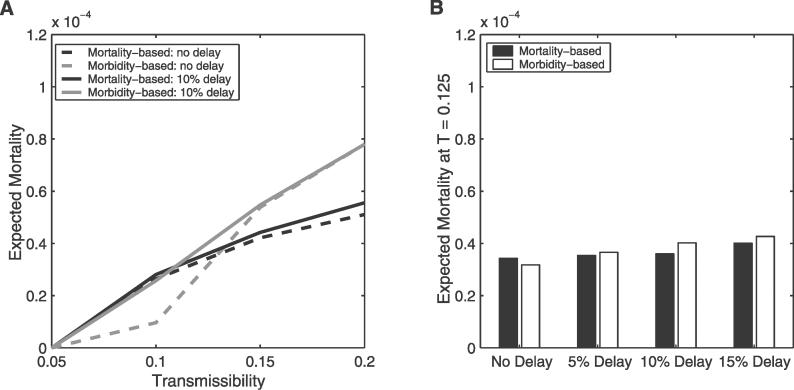
Methods and findings: We present a comparative analysis of two classes of suggested vaccination strategies: mortality-based strategies that target high-risk populations and morbidity-based strategies that target high-prevalence populations. Applying the methods of contact network epidemiology to a model of disease transmission in a large urban population, we assume that vaccine supplies are limited and then evaluate the efficacy of these strategies across a wide range of viral transmission rates and for two different age-specific mortality distributions. We find that the optimal strategy depends critically on the viral transmission level (reproductive rate) of the virus: morbidity-based strategies outperform mortality-based strategies for moderately transmissible strains, while the reverse is true for highly transmissible strains. These results hold for a range of mortality rates reported for prior influenza epidemics and pandemics. Furthermore, we show that vaccination delays and multiple introductions of disease into the community have a more detrimental impact on morbidity-based strategies than mortality-based strategies.
Conclusions: If public health officials have reasonable estimates of the viral transmission rate and the frequency of new introductions into the community prior to an outbreak, then these methods can guide the design of optimal vaccination priorities. When such information is unreliable or not available, as is often the case, this study recommends mortality-based vaccination priorities.
Conflict of interest statement
Figures
References
-
- Govaert TME, Thijs CT, Masurel N, Sprenger MJ, Dinant GJ, et al. The efficacy of influenza vaccination in elderly individuals. JAMA. 1994;272:1661–1665. - PubMed
-
- Brandriss MW, Betts RF, Mathur U, Douglas RG., Jr Responses of elderly subjects to monovalent A(HINI) and trivalent A(HINI)/A(H3N2)/B vaccines. Am Rev Respir Dis. 1981;124:681–684. - PubMed
-
- Longini IM, Koopman JS, Monto AS, Fox JP. Estimating household and community transmission parameters of influenza. Am J Epidemiol. 1982;115:736–751. - PubMed
-
- Fox JP, Hall CE, Cooney MK, Foy HM. Influenza virus infections in Seattle families, 1975–1979. Am J Epidemiol. 1982;116:212–227. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
