

Cross-sectional comparison of an automated hybrid capture 2 assay and the consensus GP5+/6+ PCR method in a population-based cervical screening program
- PMID: 17021097
- PMCID: PMC1594747
- DOI: 10.1128/JCM.02078-05
Cross-sectional comparison of an automated hybrid capture 2 assay and the consensus GP5+/6+ PCR method in a population-based cervical screening program
Abstract
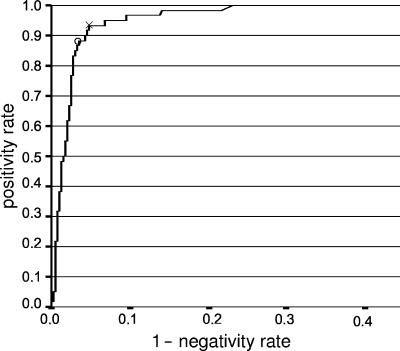
In this cross-sectional study, clinical performances of the hybrid capture 2 assay using an automated instrument (i.e., rapid capture system) (hc2-RCS) and the high-risk human papillomavirus GP5+/6+ PCR-enzyme immunoassay (EIA) test were compared using cervical scrape specimens from 8,132 women that participated in a population-based screening trial. The hc2-RCS test scored significantly more samples positive (6.8%) than the GP5+/6+ PCR-EIA (4.8%) (P < 0.0005). This could be attributed largely to a higher positivity rate by the hc2-RCS test for women with cytologically normal, borderline, or mild dyskaryosis. A receiver operator characteristics analysis of the semiquantitative hc2-RCS results in relation to different cytology categories revealed that these differences are owing to differences in assay thresholds. For women classified as having moderate dyskaryosis or worse who also had underlying histologically confirmed cervical intraepithelial neoplasia grade 3 or cervical cancer (> or =CIN3), the hc2-RCS scored 97% (31/32) of samples positive, versus 91% (29/32) by GP5+/6+ PCR-EIA. However, this difference was not significant (P = 0.25). After increasing the hc2-RCS cutoff from 1.0 to 2.0 relative light units/cutoff value of the HPV16 calibrator (RLU/CO), no additional CIN3 lesions were missed by hc2-RCS, but the number of test-positive women with normal, borderline, or mild dyskaryosis was significantly decreased (P < 0.0005). However, at this RLU/CO, the difference in test positivity between hc2-RCS and the GP5+/6+ PCR-EIA was still significant (P = 0.02). The use of an RLU/CO value of 3.0 revealed no significant difference between hc2-RCS and GP5+/6+ PCR-EIA results, and equal numbers of smears classified as > or =CIN3 (i.e., 29/32) were detected by both methods. In summary, both assays perform very well for the detection of >or =CIN3 in a population-based cervical screening setting. However, adjustment of the hc2-RCS threshold to an RLU/CO value of 2.0 or 3.0 seems to produce an improved balance between the clinical sensitivity and specificity for > or =CIN3 in population-based cervical screening.
Figures
References
-
- Berkhof, J., N. W. Bulkmans, M. C. Bleeker, S. Bulk, P. J. Snijders, F. J. Voorhorst, and C. J. Meijer. 2006. Human papillomavirus type-specific 18-month risk of high-grade cervical intraepithelial neoplasia in women with a normal or borderline/mildly dyskaryotic smear. Cancer Epidemiol. Biomarkers Prev. 15:1268-1273. - PubMed
-
- Bulkmans, N. W., M. C. Bleeker, J. Berkhof, F. J. Voorhorst, P. J. Snijders, and C. J. Meijer. 2005. Prevalence of types 16 and 33 is increased in high-risk human papillomavirus positive women with cervical intraepithelial neoplasia grade 2 or worse. Int. J. Cancer 117:177-181. - PubMed
-
- Bulkmans, N. W., L. Rozendaal, P. J. Snijders, F. J. Voorhorst, A. J. Boeke, G. R. Zandwijken, F. J. van Kemenade, R. H. Verheijen, K. Groningen, M. E. Boon, H. J. Keuning, M. van Ballegooijen, A. J. van den Brule, and C. J. Meijer. 2004. POBASCAM, a population-based randomized controlled trial for implementation of high-risk HPV testing in cervical screening: design, methods and baseline data of 44,102 women. Int. J. Cancer 110:94-101. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
