

Use of a multiantigen detection algorithm for diagnosis of Kaposi's sarcoma-associated herpesvirus infection
- PMID: 17021103
- PMCID: PMC1594766
- DOI: 10.1128/JCM.00191-06
Use of a multiantigen detection algorithm for diagnosis of Kaposi's sarcoma-associated herpesvirus infection
Abstract
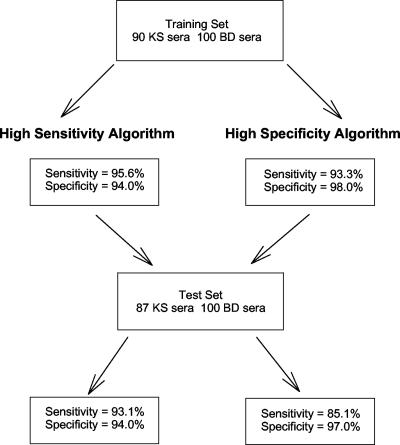
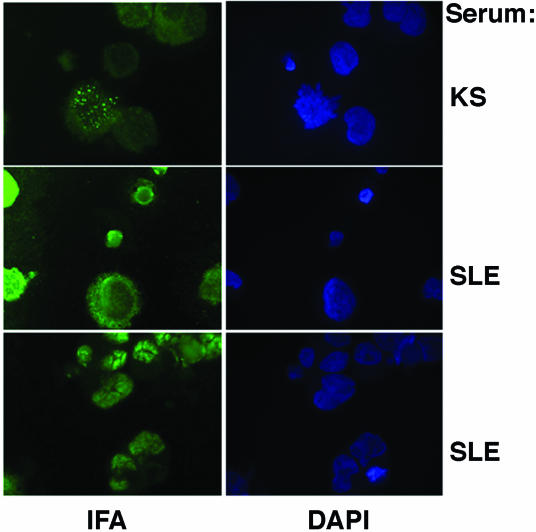
The ability to readily and accurately diagnose Kaposi's sarcoma-associated herpesvirus (KSHV, or human herpesvirus 8) infection in individuals remains a demanding task. Among the available diagnostic methods, sensitivities and specificities range widely, and many are inadequate for large-scale screening studies. We examined a serological algorithm for detecting KSHV in human sera having high sensitivity and specificity. This method uses previously described open reading frame (ORF) K8.1 and ORF65 peptide-based enzyme-linked immunosorbent assays and a novel purified recombinant full-length LANA1 protein. We generated two multiantigen algorithms: one that maximized sensitivity and one that maximized specificity. These serological algorithms were then used to evaluate seroprevalence rates among populations of clinical and epidemiological importance. The serological algorithms yielded sensitivities of 96% and 93% and specificities of 94% and 98% for the more sensitive and specific algorithms, respectively. Among kidney donors, seroprevalence was low, 4.0% (2/50), and similar to that of blood donors (P = 0.46; odds ratio [OR], 1.4; confidence interval [CI], 0.14 to 7.9) using the highly specific algorithm. Using the sensitive algorithm, 8.0% (4/50) were infected compared to 6.4% (16/250) observed among blood donors (OR, 1.3; CI, 0.41 to 4.0; P = 0.43). Among subjects requiring bone marrow transplantation, seroprevalence rates were not elevated compared to those of blood donors (OR, 2.0; 95% CI, 0.10 to 122.9; P = 0.50). Because the need for high-quality KSHV detection methods are warranted and because questions remain about the optimal methods for assessing KSHV infection in individuals, we propose a systematic approach to standardize and optimize the assessment of KSHV infection rates using a combination of established and novel serological assays and methods.
Figures


Similar articles
-
Prevalence of Kaposi's sarcoma associated herpesvirus infection measured by antibodies to recombinant capsid protein and latent immunofluorescence antigen.Lancet. 1996 Oct 26;348(9035):1133-8. doi: 10.1016/S0140-6736(96)07560-5. Lancet. 1996. PMID: 8888167
-
Comparative study of Kaposi's sarcoma-associated herpesvirus serological assays using clinically and serologically defined reference standards and latent class analysis.J Clin Microbiol. 2007 Mar;45(3):715-20. doi: 10.1128/JCM.01264-06. Epub 2006 Dec 20. J Clin Microbiol. 2007. PMID: 17182752 Free PMC article.
-
Seroprevalence of Kaposi's sarcoma-associated herpesvirus among men who have sex with men in Japan.J Med Virol. 2013 Jun;85(6):1046-52. doi: 10.1002/jmv.23558. J Med Virol. 2013. PMID: 23588730
-
Seroepidemiology of Kaposi's sarcoma-associated herpesvirus (KSHV).Semin Cancer Biol. 1999 Jun;9(3):175-85. doi: 10.1006/scbi.1998.0089. Semin Cancer Biol. 1999. PMID: 10343069 Review.
-
The Kaposi's sarcoma-associated herpesvirus (human herpesvirus-8) in Kaposi's sarcoma, malignant lymphoma, and other diseases.Ann Oncol. 1997;8 Suppl 2:123-9. Ann Oncol. 1997. PMID: 9209655 Review.
Cited by
-
Rapid Multiplexed Immunoassay for Detection of Antibodies to Kaposi's Sarcoma-Associated Herpesvirus.PLoS One. 2016 Sep 26;11(9):e0163616. doi: 10.1371/journal.pone.0163616. eCollection 2016. PLoS One. 2016. PMID: 27669509 Free PMC article.
-
Role of the Killer Immunoglobulin-like Receptor and Human Leukocyte Antigen I Complex Polymorphisms in Kaposi Sarcoma-Associated Herpesvirus Infection.Open Forum Infect Dis. 2023 Aug 18;10(8):ofad435. doi: 10.1093/ofid/ofad435. eCollection 2023 Aug. Open Forum Infect Dis. 2023. PMID: 37636520 Free PMC article.
-
Asymptomatic primary Merkel cell polyomavirus infection among adults.Emerg Infect Dis. 2011 Aug;17(8):1371-80. doi: 10.3201/eid1708.110079. Emerg Infect Dis. 2011. PMID: 21801612 Free PMC article.
-
Gender differences in Kaposi's sarcoma-associated herpesvirus infection in a population with schistosomiasis in rural China.Jpn J Infect Dis. 2012 Jul;65(4):350-3. doi: 10.7883/yoken.65.350. Jpn J Infect Dis. 2012. PMID: 22814163 Free PMC article.
-
Human Merkel cell polyomavirus infection II. MCV is a common human infection that can be detected by conformational capsid epitope immunoassays.Int J Cancer. 2009 Sep 15;125(6):1250-6. doi: 10.1002/ijc.24509. Int J Cancer. 2009. PMID: 19499548 Free PMC article.
References
-
- American Association of Blood Banks. 2005. Recieving a blood transfusion: what every patient should know. [Online.] http://www.aabb.org/Documents/Programs_and_Services/NBDRC/faqs.htm.
-
- Barozzi, P., M. Luppi, F. Facchetti, C. Mecucci, M. Alu, R. Sarid, V. Rasini, L. Ravazzini, E. Rossi, S. Festa, B. Crescenzi, D. G. Wolf, T. F. Schulz, and G. Torelli. 2003. Post-transplant Kaposi sarcoma originates from the seeding of donor-derived progenitors. Nat. Med. 9:554-561. - PubMed
-
- Biggar, R. J., E. A. Engels, D. Whitby, D. H. Kedes, and J. J. Goedert. 2003. Antibody reactivity to latent and lytic antigens to human herpesvirus-8 in longitudinally followed homosexual men. J. Infect. Dis. 187:12-18. - PubMed
-
- Blackbourn, D. J., J. Ambroziak, E. Lennette, M. Adams, B. Ramachandran, and J. A. Levy. 1997. Infectious human herpesvirus 8 in a healthy North American blood donor. Lancet 349:609-611. - PubMed
-
- Cannon, M. J., S. C. Dollard, D. K. Smith, R. S. Klein, P. Schuman, J. D. Rich, D. Vlahov, and P. E. Pellett. 2001. Blood-borne and sexual transmission of human herpesvirus 8 in women with or at risk for human immunodeficiency virus infection. N. Engl. J. Med. 344:637-643. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
