

Nutrient intake in community-dwelling adolescent girls with anorexia nervosa and in healthy adolescents
- PMID: 17023694
- PMCID: PMC3210565
- DOI: 10.1093/ajcn/84.4.698
Nutrient intake in community-dwelling adolescent girls with anorexia nervosa and in healthy adolescents
Abstract
Background: Adolescence is a common time for the onset of anorexia nervosa (AN), a condition associated with long-term medical and hormonal consequences.
Objective: The objective was to compare the nutrient intakes of community-dwelling girls with AN with those of healthy adolescents and to describe the associations between specific nutrient intakes and nutritionally dependent hormones.
Design: Nutrient intakes in 39 community-dwelling girls with AN and 39 healthy adolescents aged 12.1-18.7 y were determined by using 4-d food records. Fasting adiponectin, leptin, ghrelin, insulin, and insulin-like growth factor I (IGF-I) concentrations were measured. Indirect calorimetry was used to assess respiratory quotient and resting energy expenditure.
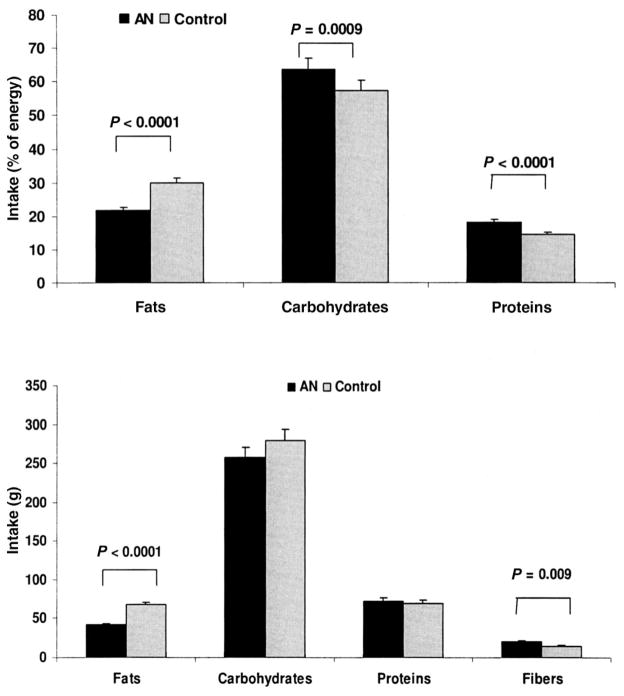
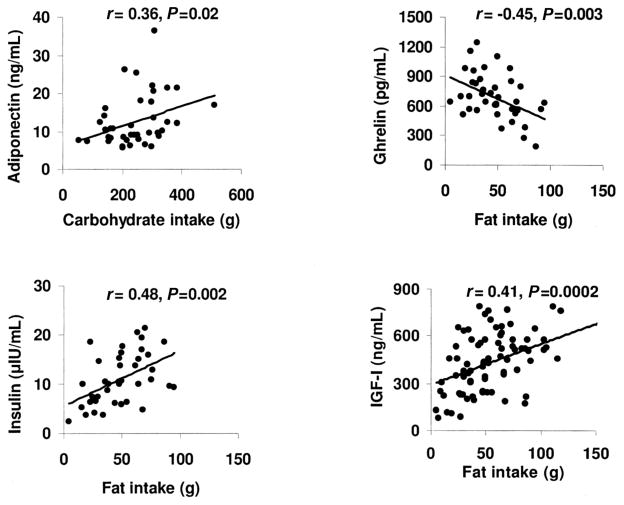
Results: In contrast with the control group, the AN group consumed fewer calories from fats (P < 0.0001) and more from carbohydrates (P = 0.0009) and proteins (P < 0.0001). Intake of individual fat components was lower and of dietary fiber higher in the AN group. No significant between-group differences were observed in dietary intakes of calcium, zinc, and iron; however, total intake was greater in the AN group because of greater supplement use (P = 0.006, 0.02, and 0.01, respectively). The AN group had greater intakes of vitamins A, D, and K and of most of the B vitamins, and significantly more girls with AN met the Dietary Reference Intake for calcium (P = 0.01) and vitamin D (P = 0.02) from supplement use. Fat intake predicted ghrelin, insulin, and IGF-I concentrations; carbohydrate intake predicted adiponectin. Resting energy expenditure was lower (P < 0.0001) and leisure activity levels higher in the AN group.
Conclusions: Despite outpatient follow-up, community-dwelling girls with AN continue to have lower fat and higher fiber intakes than do healthy adolescents, which results in lower calorie intakes. Nutritionally related hormones are associated with specific nutrient intakes.
Figures
References
-
- Whitaker A. An epidemiological study of anorectic and bulimic symptoms in adolescent girls: implications of pediatricians. Pediatr Ann. 1992;21:752–9. - PubMed
-
- Rastam M, Gillberg C, Garton M. Anorexia nervosa in a Swedish urban region. A population-based study. Br J Psychiatr. 1989;155:642–6. - PubMed
-
- Neumark-Sztainer D, Hannan P. Weight-related behaviors among adolescent girls and boys: results from a national survey. Arch Pediatr Adolesc Med. 2000;154:569–77. - PubMed
-
- Bachrach L, Guido D, Katzman D, Litt I, Marcus R. Decreased bone density in adolescent girls with anorexia nervosa. Pediatrics. 1990;86:440–7. - PubMed
-
- Kooh S, Noriega E, Leslie K, Muller C, Harrison J. Bone mass and soft tissue composition in adolescents with anorexia nervosa. Bone. 1996;19:181–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
