

Control of Schistosoma mekongi in Cambodia: results of eight years of control activities in the two endemic provinces
- PMID: 17028047
- PMCID: PMC5625998
- DOI: 10.1016/j.trstmh.2006.04.011
Control of Schistosoma mekongi in Cambodia: results of eight years of control activities in the two endemic provinces
Abstract
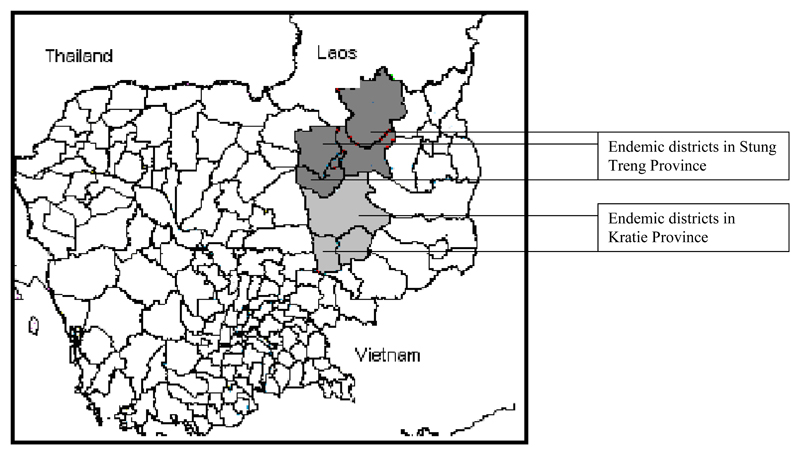
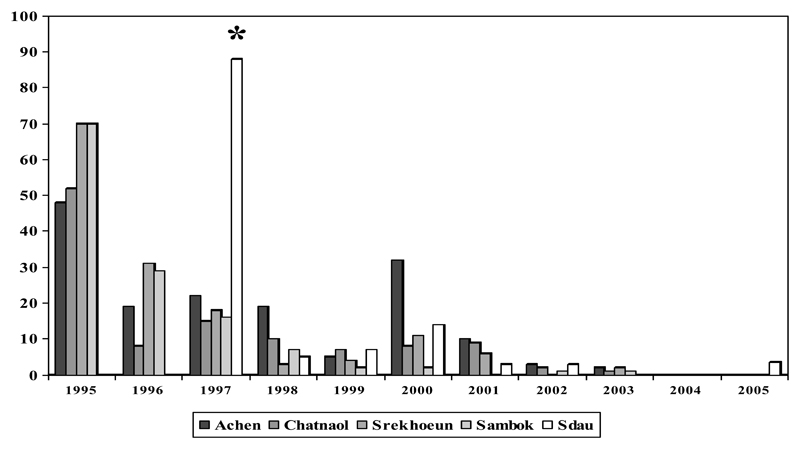
In Cambodia, schistosomiasis is transmitted in the provinces of Kratie and Stung Treng where approximately 80000 individuals are estimated to be at risk of infection. The baseline prevalence of infection was estimated to be between 73% and 88%, and cases of severe morbidity (hepatosplenomegaly, puberty retardation) and mortality were very common. In 1994, the Ministry of Health of Cambodia started schistosomiasis control applying universal chemotherapy with praziquantel (40mg/kg). The coverage of the programme was between 62% and 86% for 8 years. This simple control measure resulted in the control of the disease: no cases were reported in 2004 and only three cases were reported in 2005. In addition, there are no longer reports of cases of severe morbidity due to schistosomiasis. Since the beginning of the control programme, a single dose of mebendazole (500mg) has been combined with praziquantel during the mass chemotherapy; as a result the prevalence of Ascaris lumbricoides and hookworms dropped from 74.5% to 10% and from 86% to 40% respectively. The experience in Cambodia demonstrates that, with political commitment, control of parasitic diseases is achievable even in a situation of minimal resources. The programme represents a successful model for other developing countries.
Conflict of interest statement
The authors have no conflicts of interest concerning the work reported in this paper.
Figures
Similar articles
-
Schistosoma mekongi in Cambodia and Lao People's Democratic Republic.Adv Parasitol. 2010;72:179-203. doi: 10.1016/S0065-308X(10)72007-8. Adv Parasitol. 2010. PMID: 20624532 Review.
-
Liver morbidity due to Schistosoma mekongi in Cambodia after seven rounds of mass drug administration.Trans R Soc Trop Med Hyg. 2007 Aug;101(8):759-65. doi: 10.1016/j.trstmh.2007.04.007. Epub 2007 Jun 12. Trans R Soc Trop Med Hyg. 2007. PMID: 17568642
-
Schistosomiasis mekongi: from discovery to control.Parasitol Int. 2004 Jun;53(2):135-42. doi: 10.1016/j.parint.2004.01.004. Parasitol Int. 2004. PMID: 15081945 Review.
-
Comparison of novel and standard diagnostic tools for the detection of Schistosoma mekongi infection in Lao People's Democratic Republic and Cambodia.Infect Dis Poverty. 2017 Aug 10;6(1):127. doi: 10.1186/s40249-017-0335-x. Infect Dis Poverty. 2017. PMID: 28793922 Free PMC article.
-
Effects of repeated praziquantel treatment on schistosomiasis mekongi morbidity as detected by ultrasonography.Parasitol Int. 2006 Dec;55(4):261-5. doi: 10.1016/j.parint.2006.06.005. Epub 2006 Aug 8. Parasitol Int. 2006. PMID: 16893676
Cited by
-
Preventive chemotherapy as a strategy for elimination of neglected tropical parasitic diseases: endgame challenges.Philos Trans R Soc Lond B Biol Sci. 2013 Jun 24;368(1623):20120144. doi: 10.1098/rstb.2012.0144. Print 2013 Aug 5. Philos Trans R Soc Lond B Biol Sci. 2013. PMID: 23798692 Free PMC article.
-
Has the NTD community neglected evidence-based policy? PLOS NTDs 2013 expert commentary of the viewpoint by Nagpal S, Sinclair D, Garner P.PLoS Negl Trop Dis. 2013 Jul 11;7(7):e2299. doi: 10.1371/journal.pntd.0002299. Print 2013. PLoS Negl Trop Dis. 2013. PMID: 23875037 Free PMC article. No abstract available.
-
Ingrained: Rice farming and the risk of zoonotic spillover, examples from Cambodia.One Health. 2024 Feb 29;18:100696. doi: 10.1016/j.onehlt.2024.100696. eCollection 2024 Jun. One Health. 2024. PMID: 39010950 Free PMC article. Review.
-
Current status of human hookworm infections, ascariasis, trichuriasis, schistosomiasis mekongi and other trematodiases in Lao People's Democratic Republic.Am J Trop Med Hyg. 2014 Apr;90(4):667-9. doi: 10.4269/ajtmh.13-0636. Epub 2014 Feb 10. Am J Trop Med Hyg. 2014. PMID: 24515942 Free PMC article.
-
Current advances in serological and molecular diagnosis of Schistosoma mekongi infection.Trop Med Health. 2024 Apr 22;52(1):32. doi: 10.1186/s41182-024-00598-0. Trop Med Health. 2024. PMID: 38650044 Free PMC article. Review.
References
-
- Audebaud G, Tournier-Lasserve C, Brumpt V, Jolly M, Mazaud R, Imbert X, Bazillio R. 1st case of human schistosomiasis observed in Cambodia (Kratie area) Bull Soc Pathol Exot Filiales. 1968;61:778–784. - PubMed
-
- Biays S, Stich AHR, Odermatt P, Chan L, Yersin C, Chan M, Chaem S, Lormand J-D. Foyer de bilharziose a` Schistosoma mekongi rede´couvert au Nord du Cambodge: I. Perception culturelle de la maladie; description et suivi de 20 cas cliniques graves. Trop Med Int Health. 1999;4:662–673. - PubMed
-
- Guyatt HL, Brooker S, Donnelly CA. Can prevalence of infection in school-aged children be used as an index for assessing community prevalence? Parasitology. 1999;118(Pt 3):257–268. - PubMed
-
- Hatz C. The use of ultrasounds in schistosomiasis. Adv Parasitol. 2001;48:225–284. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
