

Expression of elevated levels of pro-inflammatory cytokines in SARS-CoV-infected ACE2+ cells in SARS patients: relation to the acute lung injury and pathogenesis of SARS
- PMID: 17031779
- PMCID: PMC7167655
- DOI: 10.1002/path.2067
Expression of elevated levels of pro-inflammatory cytokines in SARS-CoV-infected ACE2+ cells in SARS patients: relation to the acute lung injury and pathogenesis of SARS
Abstract
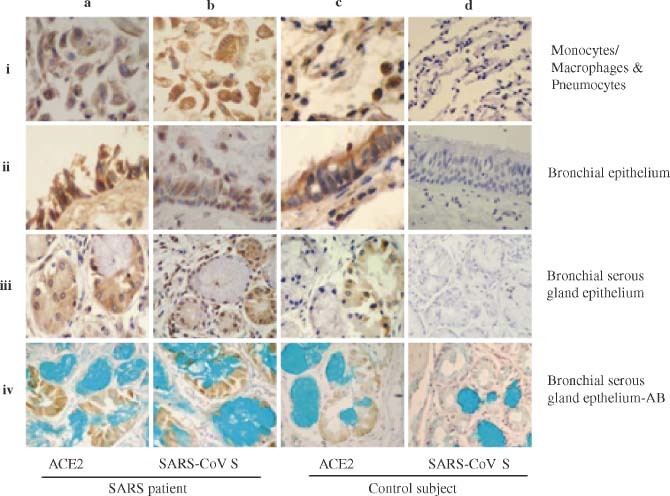
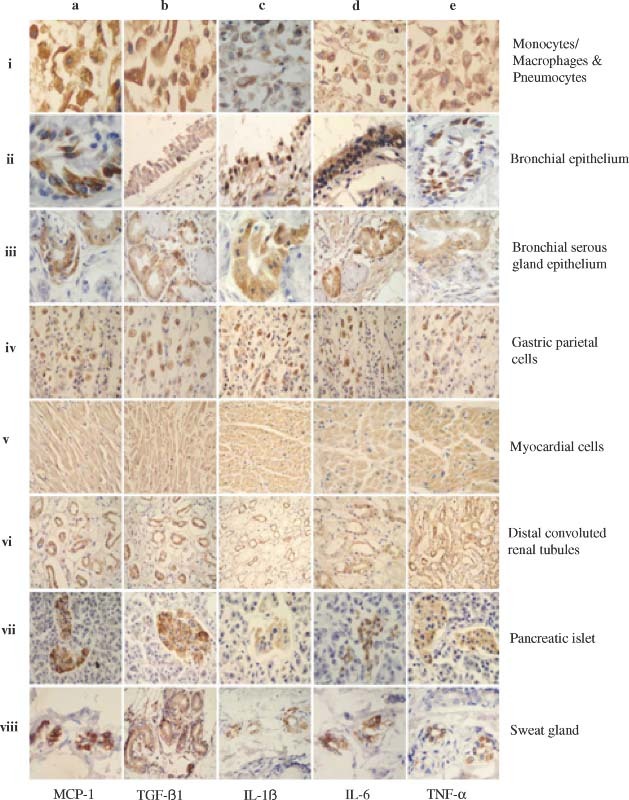
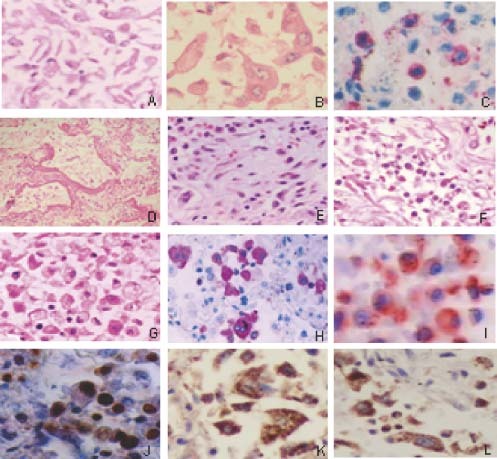
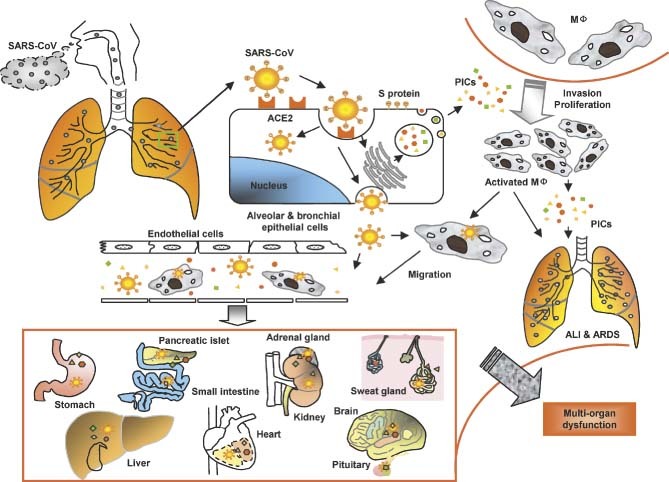
The authors have previously shown that acute lung injury (ALI) produces a wide spectrum of pathological processes in patients who die of severe acute respiratory syndrome (SARS) and that the SARS coronavirus (SARS-CoV) nucleoprotein is detectable in the lungs, and other organs and tissues, in these patients. In the present study, immunohistochemistry (IHC) and in situ hybridization (ISH) assays were used to analyse the expression of angiotensin-converting enzyme 2 (ACE2), SARS-CoV spike (S) protein, and some pro-inflammatory cytokines (PICs) including MCP-1, TGF-beta1, TNF-alpha, IL-1beta, and IL-6 in autopsy tissues from four patients who died of SARS. SARS-CoV S protein and its RNA were only detected in ACE2+ cells in the lungs and other organs, indicating that ACE2-expressing cells are the primary targets for SARS-CoV infection in vivo in humans. High levels of PICs were expressed in the SARS-CoV-infected ACE2+ cells, but not in the uninfected cells. These results suggest that cells infected by SARS-CoV produce elevated levels of PICs which may cause immuno-mediated damage to the lungs and other organs, resulting in ALI and, subsequently, multi-organ dysfunction. Therefore application of PIC antagonists may reduce the severity and mortality of SARS.
Copyright 2006 Pathological Society of Great Britain and Ireland.
Figures

References
-
- Ksiazek TG, Erdman D, Goldsmith CS, Zaki SR, Peret T, Emery S, et al. A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med 2003; 348: 1953–1966. - PubMed
-
- Drosten C, Gunther S, Preiser W, Van Der WS, Brodt HR, Becker S, et al. Identification of a novel coronavirus in patients with severe acute respiratory syndrome. N Engl J Med 2003; 348: 1967–1976. - PubMed
-
- Marra MA, Jones SJM, Astell CR, Holt RA, Brooks‐Wilson A, Butterfield YSN, et al. The genome sequence of the SARS‐associated coronavirus. Science 2003; 300: 1399–1404. - PubMed
-
- Rota PA, Oberste MS, Monroe SS, Nix WA, Campagnoli R, Icenogle JP, et al. Characterization of a novel coronavirus associated with severe acute respiratory syndrome. Science 2003; 300: 1394–1399. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
