

Magnetic resonance imaging of the fetal brain and spine: an increasingly important tool in prenatal diagnosis: part 2
- PMID: 17032846
- PMCID: PMC7977903
Magnetic resonance imaging of the fetal brain and spine: an increasingly important tool in prenatal diagnosis: part 2
Abstract
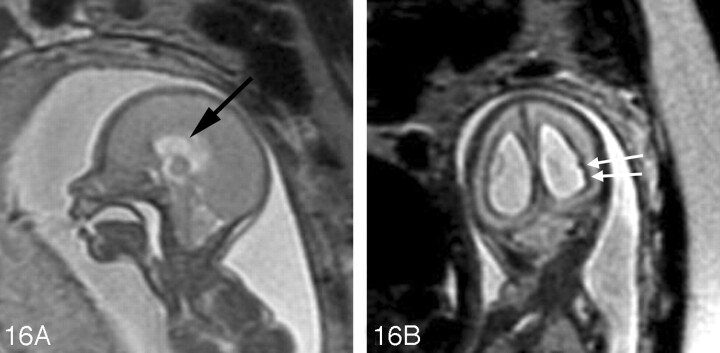
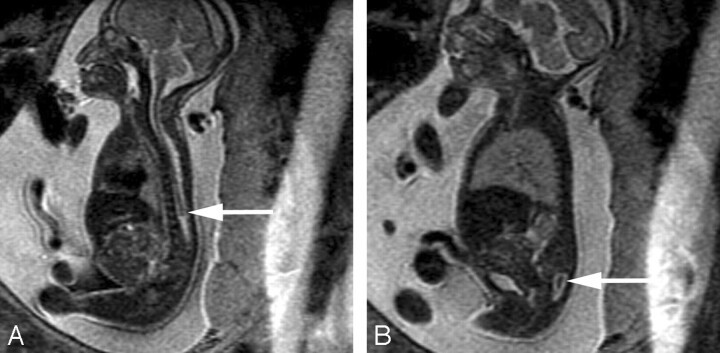
Fetal MR imaging is an increasingly available technique used to evaluate the fetal brain and spine. This is made possible by recent advances in technology, such as rapid pulse sequences, parallel imaging, and advances in coil design. This provides a unique opportunity to evaluate processes that cannot be approached by any other current imaging technique, and it affords a unique opportunity for studying in vivo brain development and early diagnosis of congenital abnormalities inadequately visualized or undetectable by prenatal sonography. This 2-part review summarizes some of the latest developments in MR imaging of the fetal brain and spine and its application to prenatal diagnosis. The first part discussed the utility, safety, and technical aspects of fetal MR imaging; the appearance of normal fetal brain development; and the role of fetal MR imaging in the evaluation of fetal ventriculomegaly. In this second part, we focus on additional clinical applications of fetal MR imaging, including suspected abnormalities of the corpus callosum, malformations of cortical development, and spine abnormalities.
Figures







References
-
- Bajoria R, Wee LY, Anwar S, et al. Outcome of twin pregnancies complicated by single intrauterine death in relation to vascular anatomy of the monochorionic placenta. Hum Reprod 1999;14:2124–30 - PubMed
-
- Barkovich AJ. Pediatric Neuroimaging. 4th ed. Philadelphia: Lippincott Williams & Wilkins,2005. .
-
- Aicardi J, Chevrie JJ, Baraton J. Agenesis of the corpus callosum. In: Vinken PJ, Bruyn GW, Klawans HL, eds. Handbook of Clinical Neurology, Revised Series, Vol. 6. New York: Elsevier Science,1987. :149–73
-
- Evangelista dos Santos AC, Midleton SR, Fonseca RL, et al. Clinical neuroimaging and cytogenetic findings in 20 patients with corpus callosum dysgenesis. Arq Neuropsiquiatr 2002;60:382–5 - PubMed
-
- Lacey DJ. Agenesis of the corpus callosum. Clinical features in 40 children. Am J Dis Child 1985;139:953–55 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical