

Symptomatic refractures after vertebroplasty in patients with steroid-induced osteoporosis
- PMID: 17032871
- PMCID: PMC7977917
Symptomatic refractures after vertebroplasty in patients with steroid-induced osteoporosis
Abstract
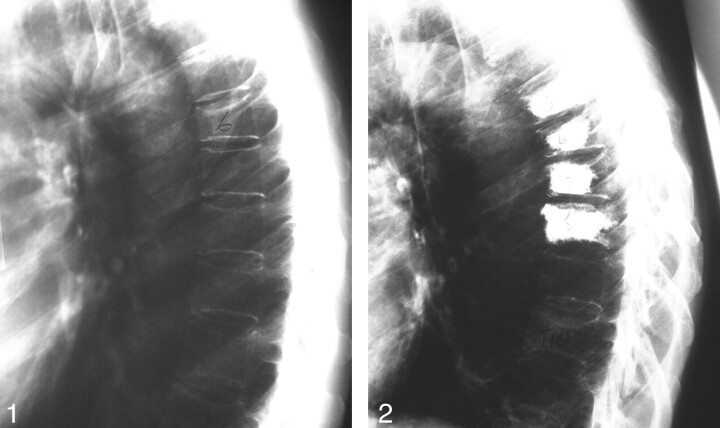
Background and purpose: Refracture after percutaneous vertebroplasty in patients receiving oral glucocorticoid therapy has caused some patients and referring physicians to have negative perceptions concerning the efficacy of the initial vertebroplasty treatment. The purpose of this study was to analyze symptomatic refractures after vertebroplasty in patients on oral steroid therapy. We hypothesized that the higher refracture rate of patients on oral glucocorticoid therapy after percutaneous vertebroplasty is due not to an inadequacy of the procedure but rather to a naturally higher predisposition of these patients to refracture compared with patients with primary osteoporosis.
Methods: A retrospective analysis was performed on all osteoporosis patients having initial vertebroplasty from August 1999 to August 2003. The follow-up period was limited to 1 year after initial vertebroplasty session, with the last follow-up date ending in August 2004. Data were collected on 387 osteoporosis patients.
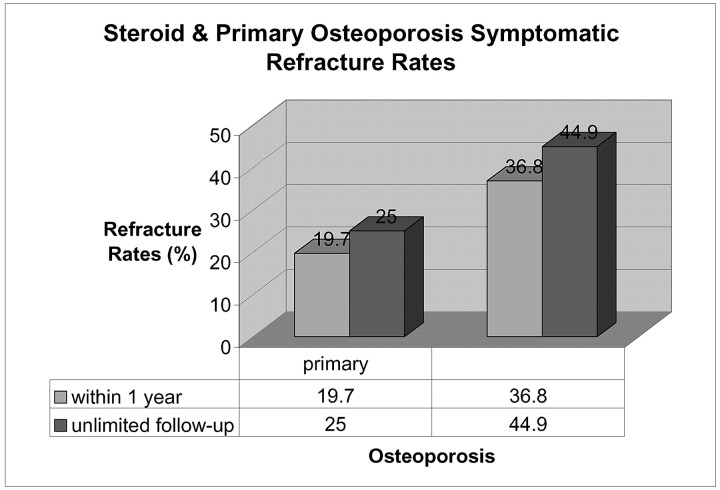
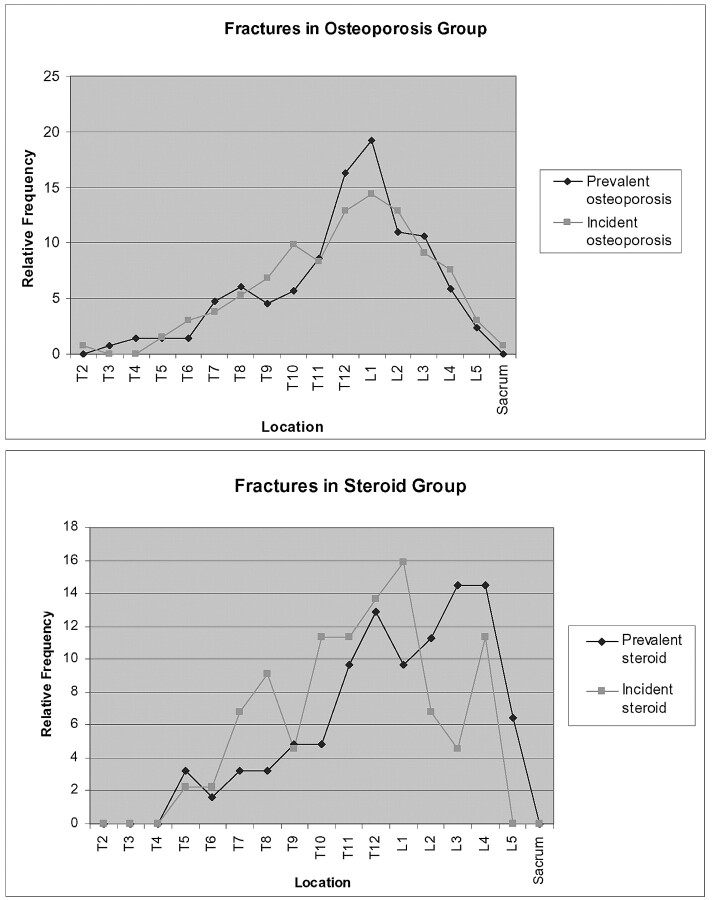
Results: Of the patients with primary osteoporosis, 20.6% patients refractured whereas 37.8% of the patients with steroid-induced osteoporosis had symptomatic refractures within 1 year of initial vertebroplasty. Relative risk of refracture within 1 year for the patients with steroid-induced osteoporosis was 1.84 compared with the patients with primary osteoporosis. In addition, the patients with steroid-induced osteoporosis were more likely to refracture after their second treatment session (within 1 year of initial vertebroplasty) than those with primary osteoporosis.
Conclusion: Patients presenting on oral steroid therapy at their initial vertebroplasty are almost twice more likely to have symptomatic refractures than primary osteoporosis patients within 1 year of initial vertebroplasty.
Figures
References
-
- Hide IG, Gangi A. Percutaneous vertebroplasty: history, technique and current perspectives. Clin Radiol 2004;59:461–67 - PubMed
-
- Chiras J, Depriester C, Weill A, et al. Vertebroplasties purcutanees. J Neuroradiol 1997;24:45–49 - PubMed
-
- Martin JB, Jean B, Sugui K, et al. Vertebroplasty: clinical experience and follow-up results. Bone 1999;25(suppl):11S–15S - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical