

Microscopic-observation drug-susceptibility assay for the diagnosis of TB
- PMID: 17035648
- PMCID: PMC1780278
- DOI: 10.1056/NEJMoa055524
Microscopic-observation drug-susceptibility assay for the diagnosis of TB
Abstract
Background: New diagnostic tools are urgently needed to interrupt the transmission of tuberculosis and multidrug-resistant tuberculosis. Rapid, sensitive detection of tuberculosis and multidrug-resistant tuberculosis in sputum has been demonstrated in proof-of-principle studies of the microscopic-observation drug-susceptibility (MODS) assay, in which broth cultures are examined microscopically to detect characteristic growth.
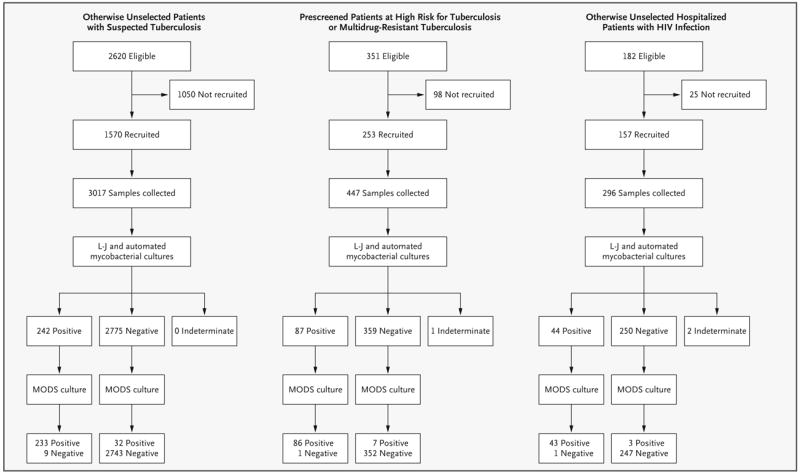
Methods: In an operational setting in Peru, we investigated the performance of the MODS assay for culture and drug-susceptibility testing in three target groups: unselected patients with suspected tuberculosis, prescreened patients at high risk for tuberculosis or multidrug-resistant tuberculosis, and unselected hospitalized patients infected with the human immunodeficiency virus. We compared the MODS assay head-to-head with two reference methods: automated mycobacterial culture and culture on Löwenstein-Jensen medium with the proportion method.
Results: Of 3760 sputum samples, 401 (10.7%) yielded cultures positive for Mycobacterium tuberculosis. Sensitivity of detection was 97.8% for MODS culture, 89.0% for automated mycobacterial culture, and 84.0% for Löwenstein-Jensen culture (P<0.001); the median time to culture positivity was 7 days, 13 days, and 26 days, respectively (P<0.001), and the median time to the results of susceptibility tests was 7 days, 22 days, and 68 days, respectively. The incremental benefit of a second MODS culture was minimal, particularly in patients at high risk for tuberculosis or multidrug-resistant tuberculosis. Agreement between MODS and the reference standard for susceptibility was 100% for rifampin, 97% for isoniazid, 99% for rifampin and isoniazid (combined results for multidrug resistance), 95% for ethambutol, and 92% for streptomycin (kappa values, 1.0, 0.89, 0.93, 0.71, and 0.72, respectively).
Conclusions: A single MODS culture of a sputum sample offers more rapid and sensitive detection of tuberculosis and multidrug-resistant tuberculosis than the existing gold-standard methods used.
Copyright 2006 Massachusetts Medical Society.
Figures


Comment in
-
Rapid detection of tuberculosis and drug-resistant tuberculosis.N Engl J Med. 2006 Oct 12;355(15):1606-8. doi: 10.1056/NEJMe068173. N Engl J Med. 2006. PMID: 17035655 No abstract available.
-
MODS assay for the diagnosis of TB.N Engl J Med. 2007 Jan 11;356(2):188; author reply 189. doi: 10.1056/NEJMc063088. N Engl J Med. 2007. PMID: 17215539 No abstract available.
-
MODS assay for the diagnosis of TB.N Engl J Med. 2007 Jan 11;356(2):188; author reply 189. N Engl J Med. 2007. PMID: 17225284 No abstract available.
-
Microscopic-observation drug-susceptibility assay was more sensitive than standard tests for diagnosing tuberculosis.ACP J Club. 2007 Mar-Apr;146(2):45. ACP J Club. 2007. PMID: 17335168 No abstract available.
References
-
- Global tuberculosis control: surveillance, planning, financing. Geneva: World Health Organization. 2006. [Accessed September 15, 2006]. pp. 1–242. http://www.who.int/tb/publications/global_report/2006/en/index.html.
-
- The global plan to stop TB, 2006–2015 Geneva. Stop TB Partnership and World Health Organization. 2006. [Accessed September 15, 2006]. pp. 1–172. http://www.stoptb.org/globalplan.
-
- Espinal MA, Kim SJ, Suarez PG, et al. Standard short-course chemotherapy for drug-resistant tuberculosis: treatment outcomes in 6 countries. JAMA. 2000;283:2537–45. - PubMed
-
- Chavez Pachas AM, Blank R, Smith Fawzi MC, Bayona J, Becerra MC, Mitnick CD. Identifying early treatment failure on category I therapy for pulmonary tuberculosis in Lima Ciudad, Peru. Int J Tuberc Lung Dis. 2004;8:52–8. - PubMed
-
- Dowdy DW, Chaisson RE, Moulton LH, Dorman SE. The potential impact of enhanced diagnostic techniques for tuberculosis driven by HIV: a mathematical model. AIDS. 2006;20:751–62. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical