

Human bocavirus infection in young children in the United States: molecular epidemiological profile and clinical characteristics of a newly emerging respiratory virus
- PMID: 17041854
- PMCID: PMC7204143
- DOI: 10.1086/508213
Human bocavirus infection in young children in the United States: molecular epidemiological profile and clinical characteristics of a newly emerging respiratory virus
Abstract
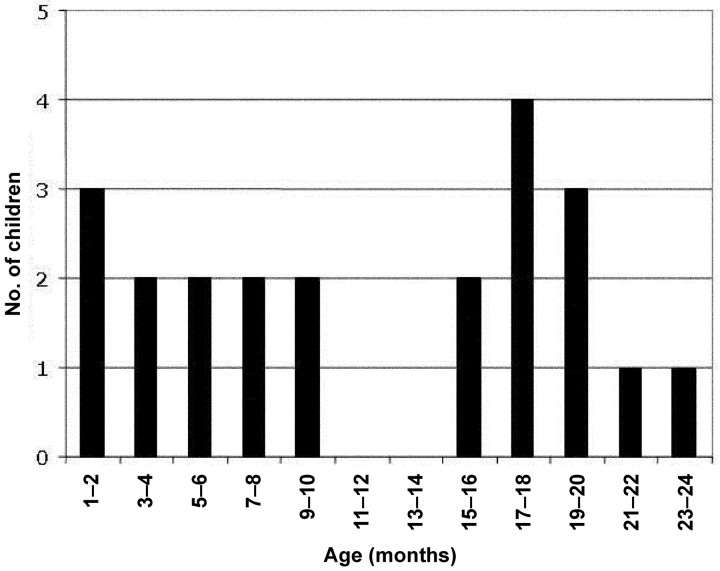
Background: Human bocavirus (HBoV) is a newly identified human parvovirus that was originally identified in the respiratory secretions of children with respiratory tract disease. To further investigate the epidemiological profile and clinical characteristics of HBoV infection, we screened infants and children <2 years of age (hereafter referred to as "children") for HBoV.
Methods: Children for whom respiratory specimens submitted to a diagnostic laboratory tested negative for respiratory syncytial virus, parainfluenza viruses (types 1-3), influenza A and B viruses, and adenovirus, as well as asymptomatic children, underwent screening for HBoV by use of polymerase chain reaction (PCR). Respiratory specimens were obtained from the children from 1 January 2004 through 31 December 2004.
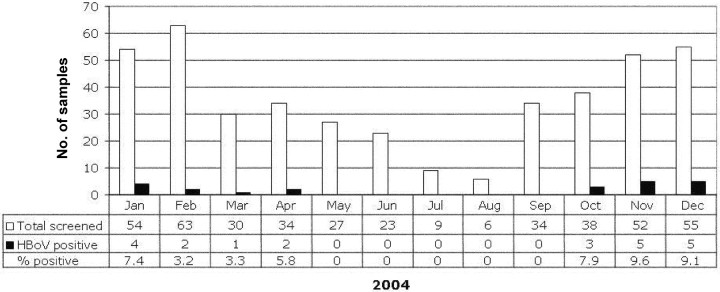
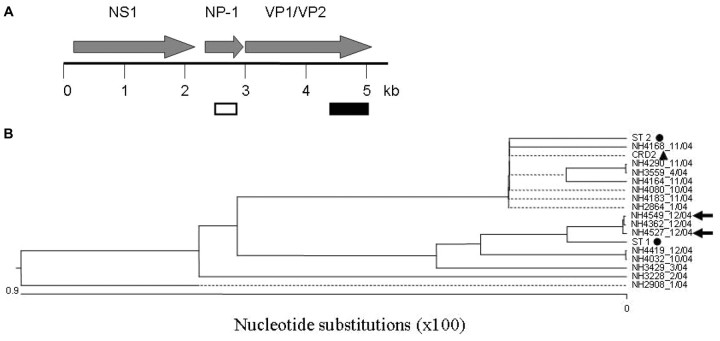
Results: Twenty-two (5.2%) of the 425 children who had a respiratory specimen submitted to the diagnostic laboratory and 0 of the 96 asymptomatic children were found to be positive for HBoV by PCR (P=.02). Fever, rhinorrhea, cough, and wheezing were observed in > or =50% of the HBoV-positive children. Of the 17 children who had chest radiography performed, 12 (70.6%) had abnormal findings. HBoV appeared to have a seasonal distribution. Nucleotide polymorphisms were detected in the viral capsid protein (VP) 1/VP2 genes. Two distinct HBoV genotypes circulated during the study period.
Conclusions: HBoV is circulating in the United States and is associated with both upper and lower respiratory tract disease in infants and young children.
Figures

Comment in
-
Human bocavirus: developing evidence for pathogenicity.J Infect Dis. 2006 Nov 1;194(9):1197-9. doi: 10.1086/508228. Epub 2006 Sep 26. J Infect Dis. 2006. PMID: 17041844 Free PMC article. No abstract available.
References
-
- Murray C, Lopez A, Mathers C, Stein C. Global programme on evidence for health policy. Geneva: World Health Organization; 2001. The Global Burden of Disease 2000 Project: aims, methods and data sources.
-
- Davies HD, Matlow A, Petric M, Glazier R, Wang EE. Prospective comparative study of viral, bacterial and atypical organisms identified in pneumonia and bronchiolitis in hospitalized Canadian infants. Pediatr Infect Dis J. 1996;15:371–5. - PubMed
-
- Wright AL, Taussig LM, Ray CG, Harrison HR, Holberg CJ. The Tucson Children’s Respiratory Study. II. Lower respiratory tract illness in the first year of life. Am J Epidemiol. 1989;129:1232–46. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
