

The treatment for multilevel noncontiguous spinal fractures
- PMID: 17043863
- PMCID: PMC2266655
- DOI: 10.1007/s00264-006-0241-5
The treatment for multilevel noncontiguous spinal fractures
Abstract
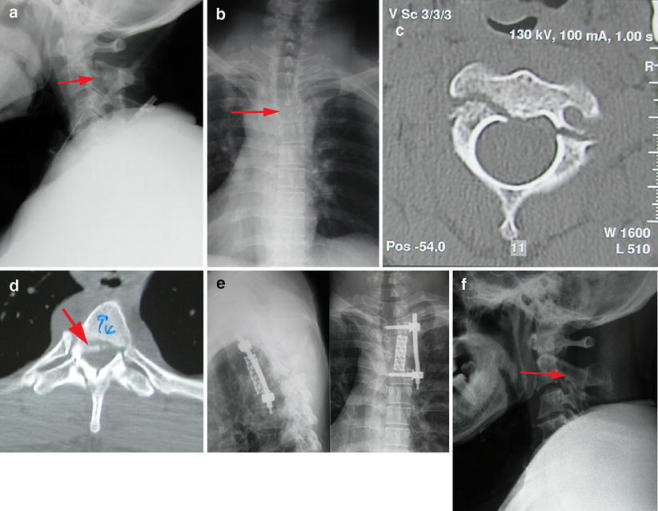
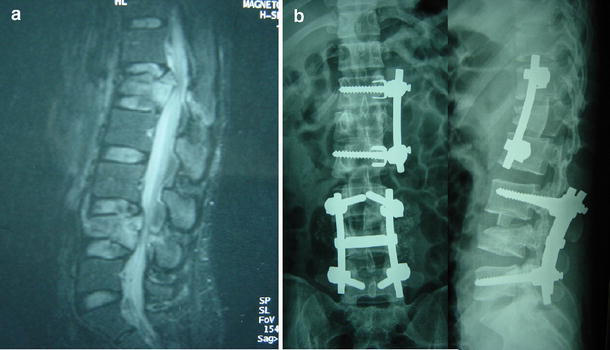
We report the outcome of 30 patients with multilevel noncontiguous spinal fractures treated between 2000 and 2005. Ten cases were treated conservatively (group A), eight cases were operated on at only one level (group B), and 12 cases were treated surgically at both levels (group C). All cases were followed up for 14-60 months (mean 32 months). Initial mobilisation with a wheelchair or crutches in group A was 9.2 +/- 1.1 weeks, which was significantly longer than groups B and C with 6.8+/-0.7 weeks and 3.1 +/- 0.4 weeks, respectively. Operative time and blood loss in group C were significantly more than group B. The neurological deficit improved in six cases in group A (60%), six in group B (75%) and eight in group C (80%). Correction of kyphotic deformity was significantly superior in groups C and B at the operated level, and increasing deformity occurred in groups A and B at the non-operated level. From the results we believe that three treatment strategies were suitable for multilevel noncontiguous spinal fractures, and individualised treatment should be used in these patients. In the patients treated surgically, the clinical and radiographic outcomes are much better.
Nous rapportons l’évolution de 30 patients avec des fractures étagées non contiguës du rachis traités entre 2000 et 2005 : 10 cas étaient traités conservativement (groupe A), 8 cas étaient opérés à un seul étage (groupe B), et 12 cas étaient opérés à plusieurs étages. Le suivi était de 14 à 60 mois (moyenne 32 mois). La mobilisation initiale, en chaise roulante ou avec des cannes, était significativement plus tardive que dans les groupes B et C. La durée opératoire et la perte de sang étaient plus importante dans le groupe C que dans le groupe B. Le déficit neurologique était amélioré dans 6 cas du groupe A (60%), 6 du groupe B (75%) et 8 du groupe C (80%). La correction de la cyphose était meilleure dans le groupe C et au niveau traité du groupe B tandis qu’une aggravation de la déformation était notée dans le groupe A et au niveau non opéré du groupe B. De ces résultats nous concluons que les trois traitements sont possibles mais qu’ils doivent être individualisés selon les patients. Les résultats cliniques et radiologiques sont meilleurs chez les patients opérés.
Figures
References
-
- Bracken MB, Shepard MJ, Collins WF et al (1990) A randomized, controlled trial of methylprednisolone or naloxone in the treatment of acute spinal-cord injury. Results of the second National Acute Spinal Cord Injury study. N Engl J Med 322:1405–1411 - PubMed
-
- Bracken MB, Shepard MJ, Collins WF et al (1992) Methylprednisolone or naxolone treatment after acute spinal cord injury: 1-year follow-up data: Results of the second National Acute Spinal Cord Injury study. J Neurosurg 76:23–31 - PubMed
-
- Cobb JR (1948) Outline for the study of scoliosis: instructional course lecture 5. Edwards, Ann Arbor, MI
-
- Ditunno JF Jr, Young W, Donovan WH et al (1994) The international standards booklet for neurological and functional classification of spinal cord injury: American Spinal Injury Association. Paraparaplegia 32:70–80 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
