

Motor field sensitivity for preoperative localization of motor cortex
- PMID: 17044563
- PMCID: PMC4045015
- DOI: 10.3171/jns.2006.105.4.588
Motor field sensitivity for preoperative localization of motor cortex
Abstract
Object: In this study the role of magnetic source imaging for preoperative motor mapping was evaluated by using a single-dipole localization method to analyze motor field data in 41 patients.
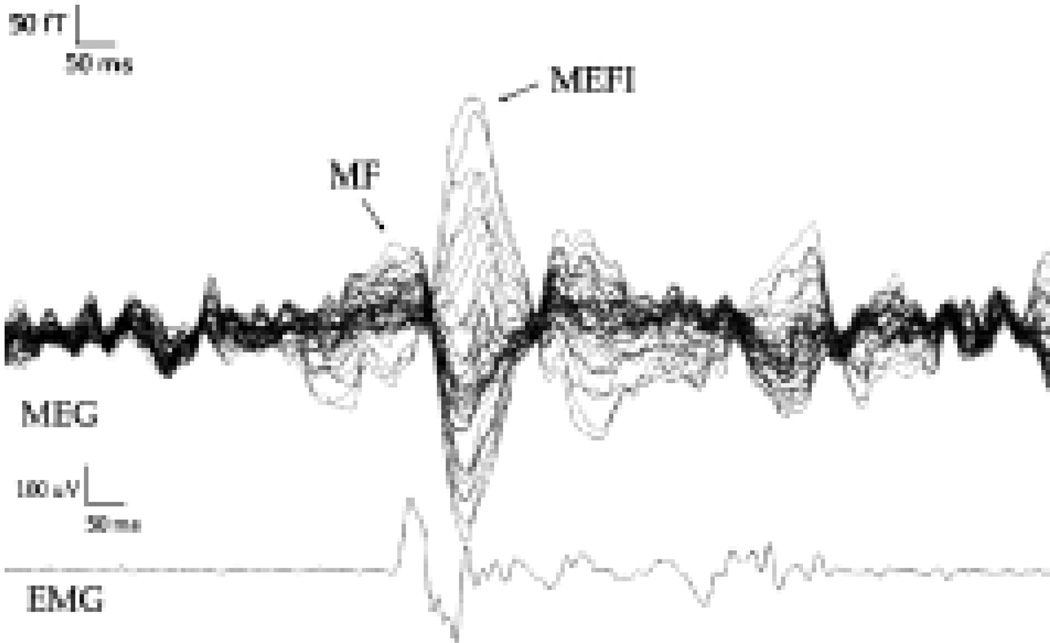
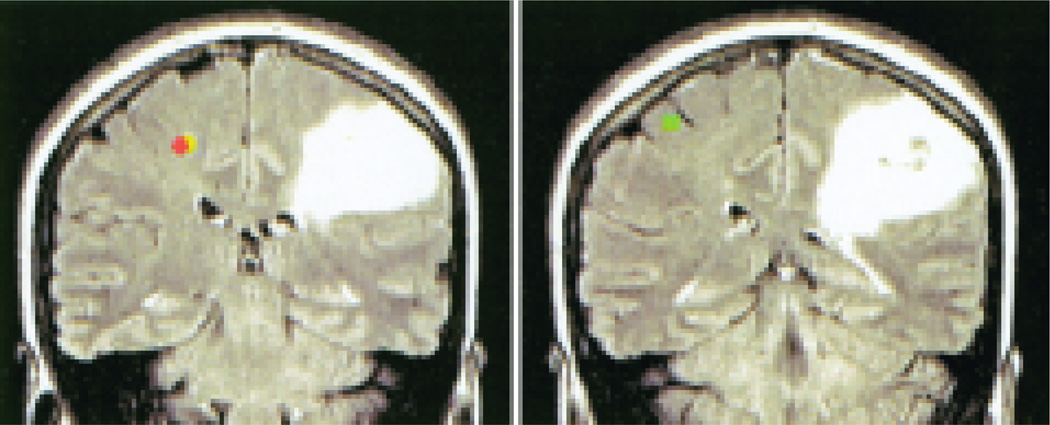
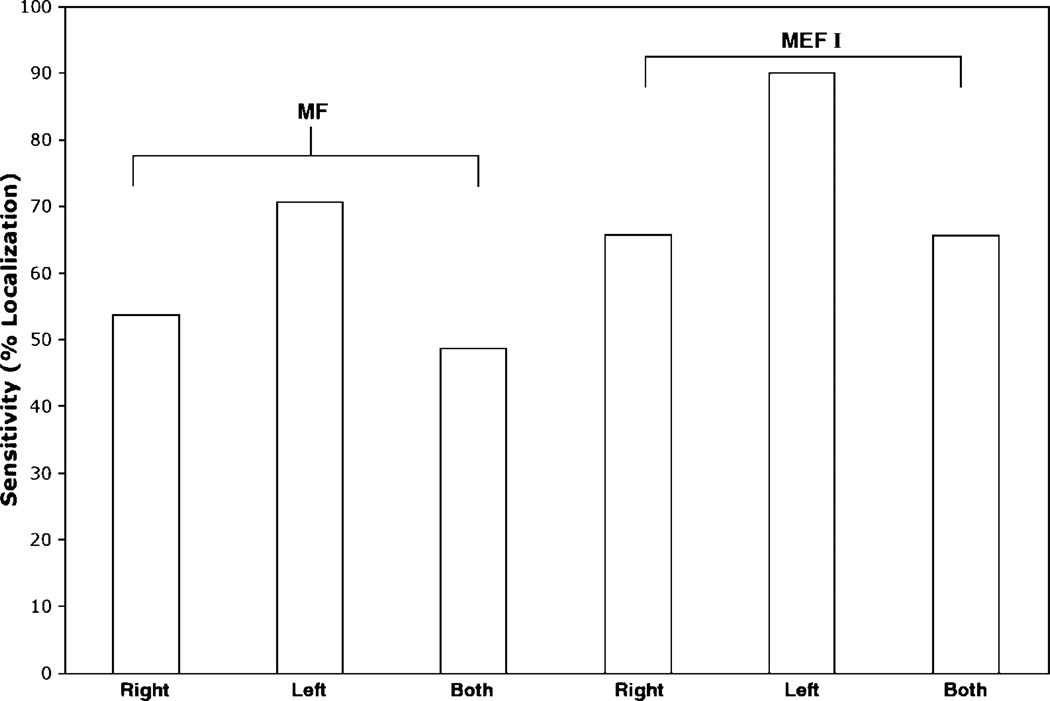
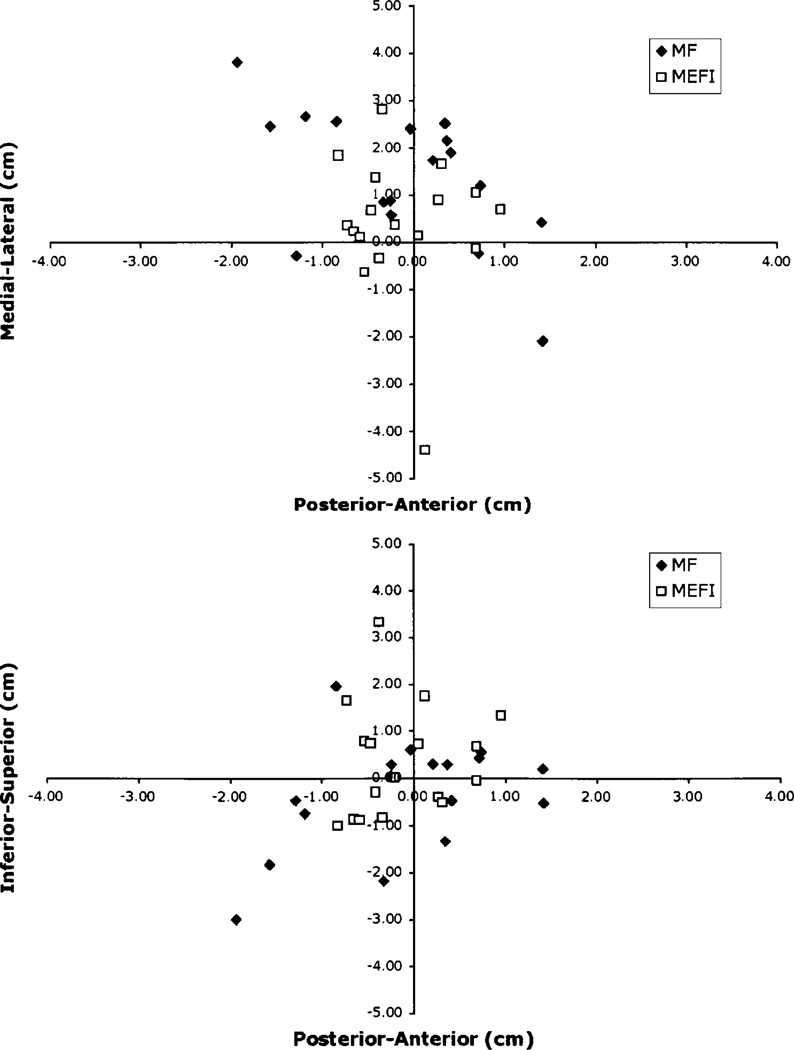
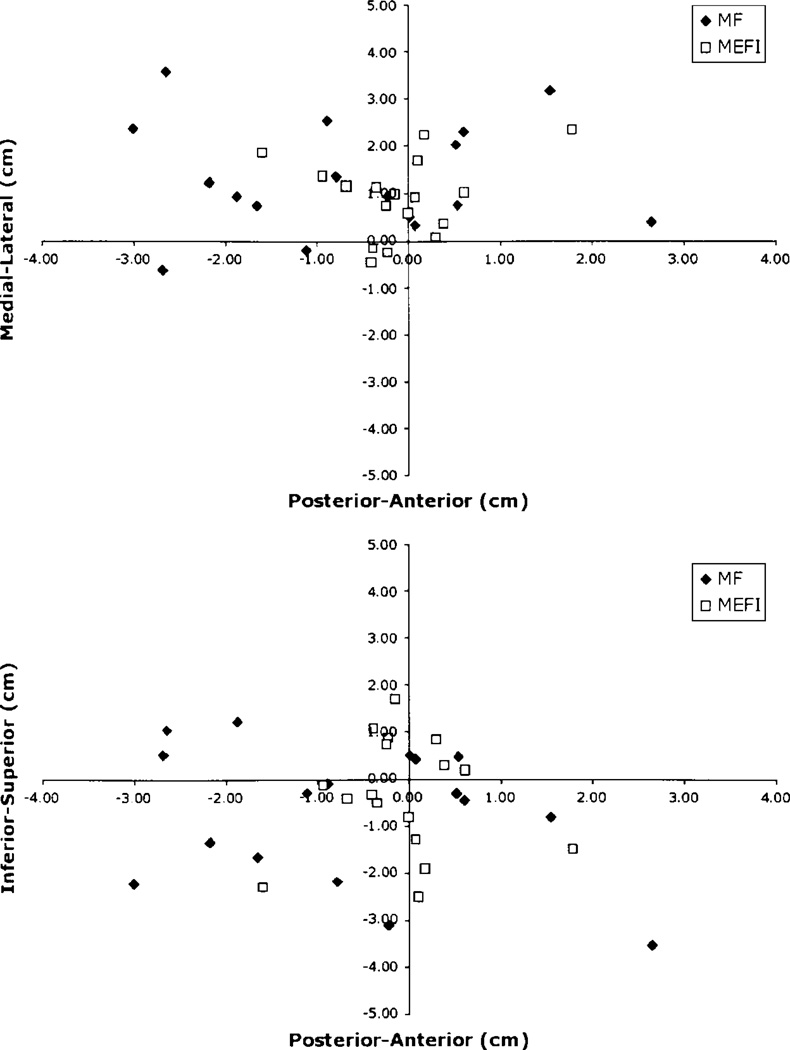
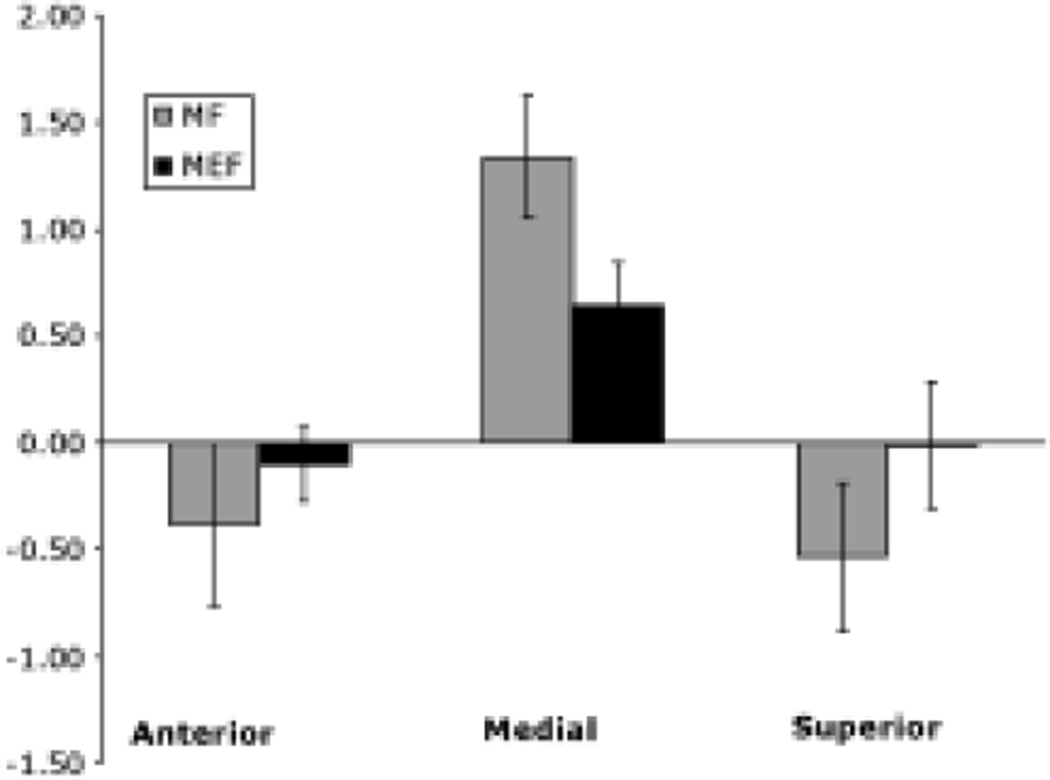
Methods: Data from affected and unaffected hemispheres were collected in patients performing voluntary finger flexion movements. Somatosensory evoked field (SSEF) data were also obtained using tactile stimulation. Dipole localization using motor field (MF) data was successful in only 49% of patients, whereas localization with movement-evoked field (MEF) data was successful in 66% of patients. When the spatial distribution of MF and MEF dipoles in relation to SSEF dipoles was analyzed, the motor dipoles were not spatially distinct from somatosensory dipoles.
Conclusions: The findings in this study suggest that single-dipole localization for the analysis of motor data is not sufficiently sensitive and is nonspecific, and thus not clinically useful.
Figures
References
-
- Castillo EM, Simos PG, Wheless JW, Baumgartner JE, Breier JI, Billingsley RL, et al. Integrating sensory and motor mapping in a comprehensive MEG protocol: clinical validity and replicability. Neuroimage. 2004;21:973–983. - PubMed
-
- Deecke L, Weinberg H, Brickett P. Magnetic fields of the human brain accompanying voluntary movement: Bereitschaftsmagnetfeld. Exp Brain Res. 1982;48:144–148. - PubMed
-
- Ebmeier K, Haberland N, Steenbeck J, Hochstetter A, Kalff R. Neuronavigation and magnetic source imaging in brain tumors. Front Radiat Ther Oncol. 1999;33:78–87. - PubMed
-
- Gallen CC, Schwartz BJ, Bucholz RD, Malik G, Barkley GL, Smith J, et al. Presurgical localization of functional cortex using magnetic source imaging. J Neurosurg. 1995;82:988–994. - PubMed
-
- Ganslandt O, Buchfelder M, Hastreiter P, Grummich P, Fahlbusch R, Nimsky C. Magnetic source imaging supports clinical decision making in glioma patients. Clin Neurol Neurosurg. 2004;107:20–26. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
