

The total mesorectal excision specimen for rectal cancer: a review of its pathological assessment
- PMID: 17046842
- PMCID: PMC1994509
- DOI: 10.1136/jcp.2006.043802
The total mesorectal excision specimen for rectal cancer: a review of its pathological assessment
Abstract
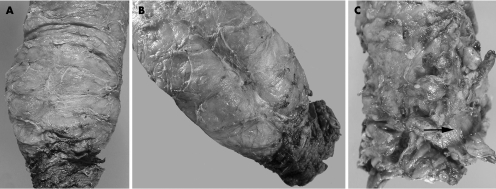
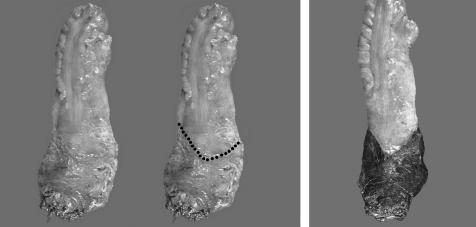
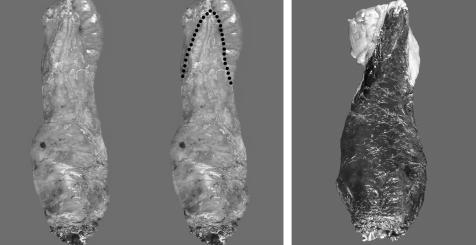
Total mesorectal excision (TME) refers to the surgical removal of the complete perirectal soft tissue envelope, using sharp instruments under direct vision, and has become the contemporary standard of care for patients with rectal cancer. Pathologists play a key role in the evaluation of these specimens, including the quality assurance of surgical performance, as well as evaluation of the circumferential radial margin (CRM). While the latter is the most significant predictor of local recurrence, the quality of the excised mesorectum is another important factor in assessing the risk of local recurrence in patients with a negative CRM. Since proper pathological assessment of the TME specimen provides important prognostic information, as well as critical feedback to surgeons regarding technical performance, it is important to have adequate guidelines for the macroscopic handling of these specimens. The CLASSICC study of the Medical Research Council in the United Kingdom, as well as the Dutch TME trial have introduced a new standard for the pathological assessment of TME specimens, including an approach that involves assessment in both the fresh and fixed states, at least 48 hours of fixation of an intact specimen, with observations made on both the external appearance and cross-sectional slices. This article reviews the pathological assessment of the TME specimen, including basic definitions, current international guidelines, an approach to evaluating the mesorectum and a discussion of special issues relating to margins, lymph node retrieval and effects of neoadjuvant therapy.
Conflict of interest statement
Competing interests: None declared.


References
-
- Heald R J, Ryall R D. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 198611479–1482. - PubMed
-
- MacFarlane J K, Ryall R D, Heald R J. Mesorectal excision for rectal cancer. Lancet 1993341457–460. - PubMed
-
- Cecil T D, Sexton R, Moran B J.et al Total mesorectal excision results in low local recurrence rates in lymph node‐positive rectal cancer. Dis Colon Rectum 2004471145–1150. - PubMed
-
- Faerden A E, Naimy N, Wiik P.et al Total mesorectal excision for rectal cancer: difference in outcome for low and high rectal cancer. Dis Colon Rectum 2005482224–2231. - PubMed
-
- Hermanek P, Hermanek P, Klimpfinger M.et al The pathological assessment of mesorectal excision: implications for further treatment and quality management. In J Colorectal Dis 200318335–341. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical