

A segmental radiological study of the spine and rib--cage in children with progressive infantile idiopathic scoliosis
- PMID: 17049098
- PMCID: PMC1635062
- DOI: 10.1186/1748-7161-1-17
A segmental radiological study of the spine and rib--cage in children with progressive infantile idiopathic scoliosis
Abstract
Background: The role of rib cage in the development of progressive infantile idiopathic scoliosis (IIS) has not been studied previously. No report was found for rib growth in children with IIS. These findings caused us to undertake a segmental radiological study of the spine and rib-cage in children with progressive IIS. The aim of the present study is to present a new method for assessing the thoracic shape in scoliotics and in control subjects and to compare the findings between the two groups.
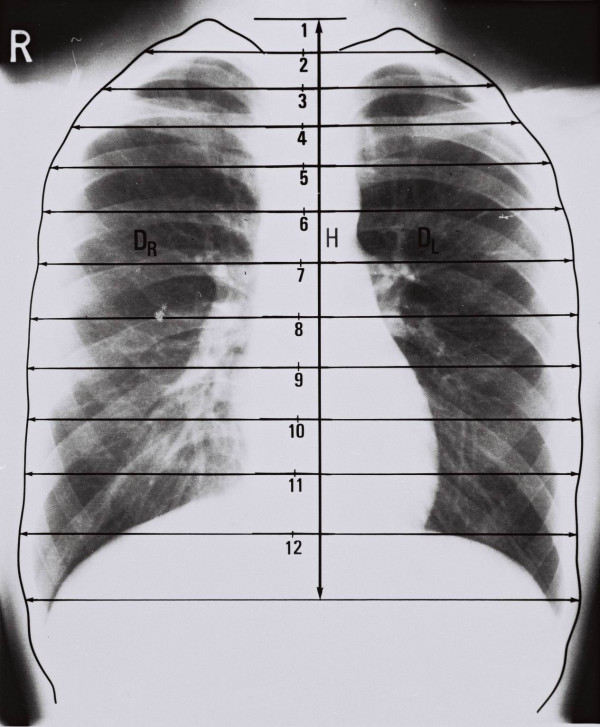
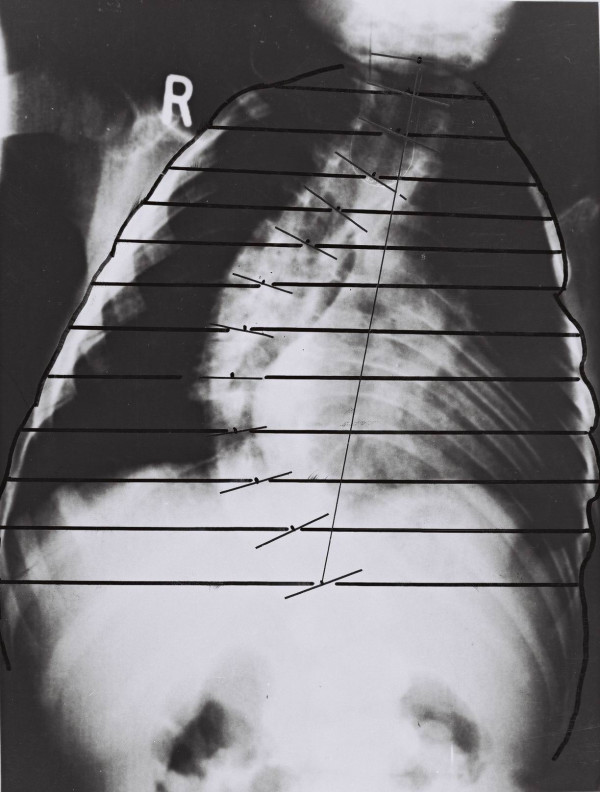
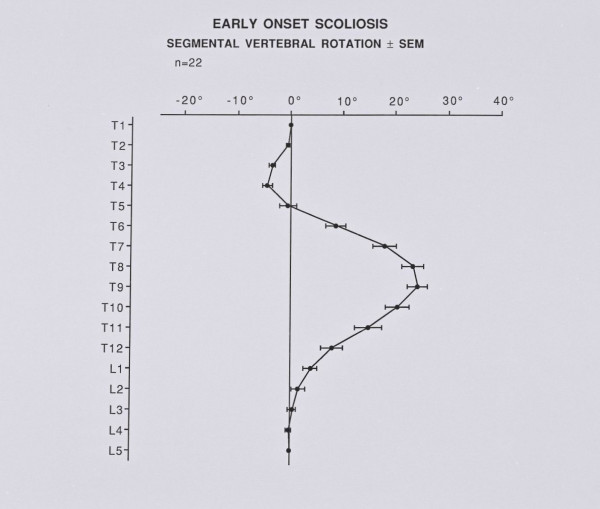
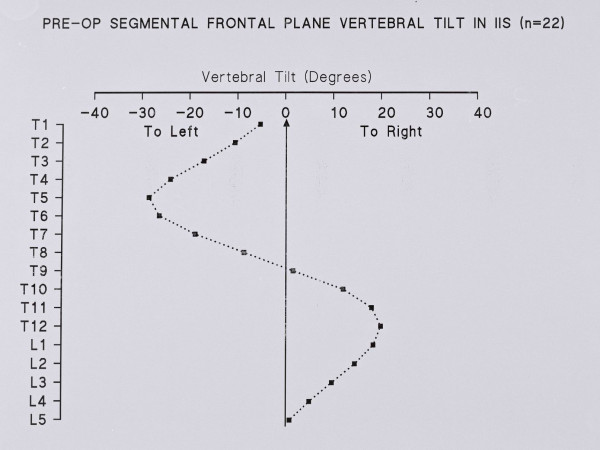
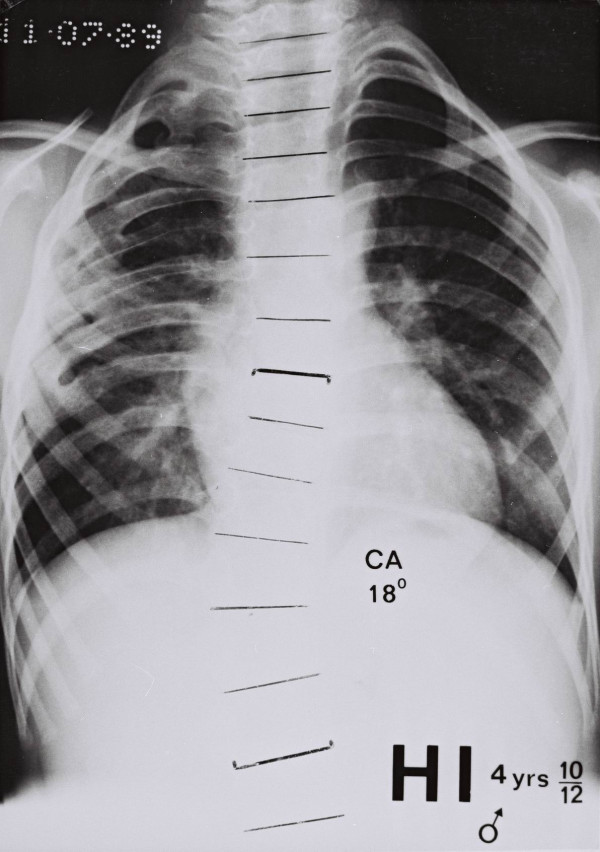
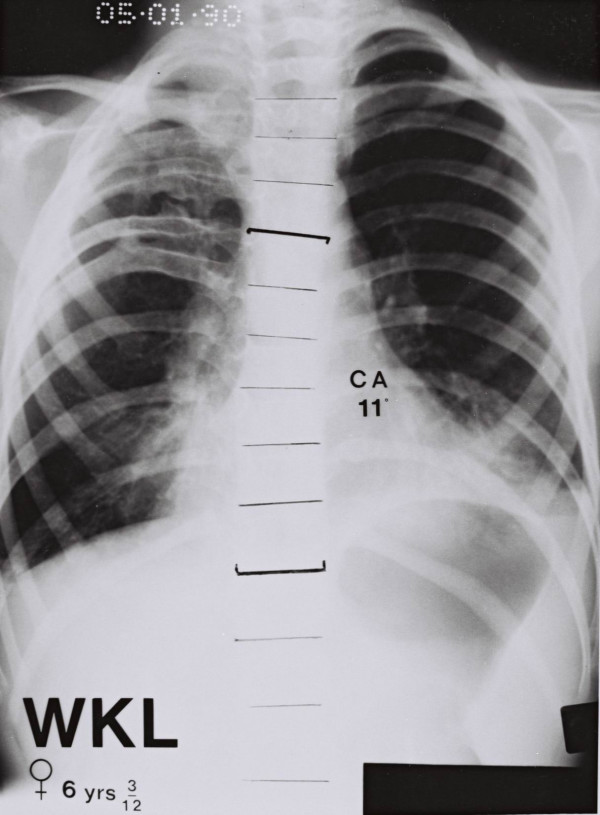
Materials and methods: In the posteroanterior (PA) spinal radiographs of 24 patients with progressive IIS, with a mean age of 4.1 years old, the Thoracic Ratios (TRs) (segmental convex and concave TRs), the Cobb angle, the segmental vertebral rotation and vertebral tilt were measured. In 233 subjects, with a mean age of 5.1 years old, who were used as a control group, the segmental left and right TRs and the total width of the chest (left plus right TRs) were measured in PA chest radiographs. Statistical analysis included Mann-Whitney, Spearman correlation coefficient, multiple linear regression analysis and ANOVA.
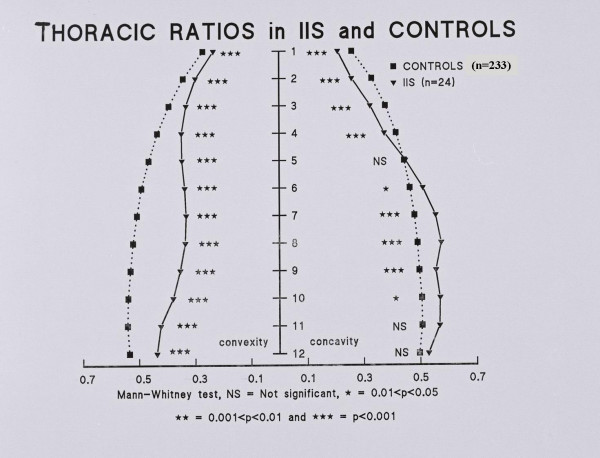
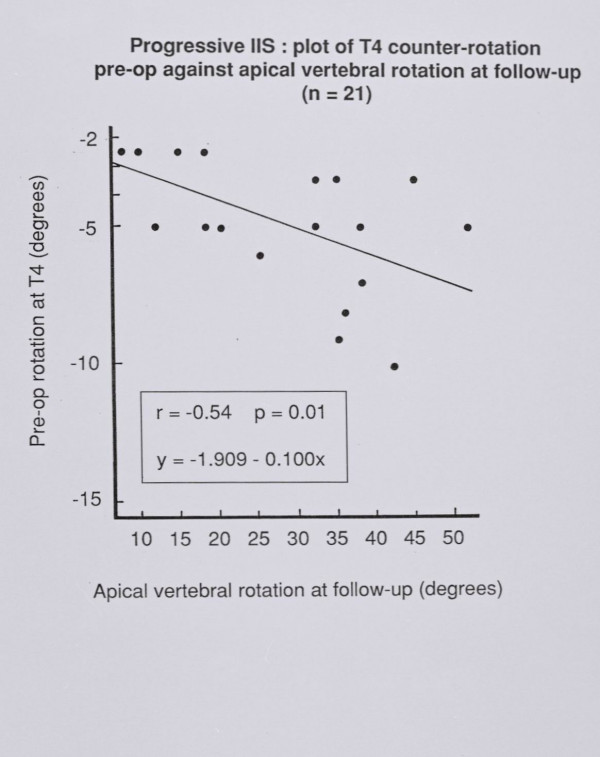
Results: The comparison shows that the scoliotic thorax is significantly narrower than that of the controls at all spinal levels. The upper chest in IIS is funnel-shaped and the vertebral rotation at T4 early in management correlates significantly with the apical vertebral rotation at follow up.
Conclusion: The IIS thorax is narrower than that of the controls, the upper chest is funnel-shaped and there is a predictive value of vertebral rotation at the upper limit of the thoracic curve of IIS, which reflects, impaired rib control of spinal rotation possibly due to neuromuscular factors, which contribute also to the funnel-shaped chest.
Figures
References
-
- Grivas TB, Webb JK, Burwell RG. Arrest of curve progression by epiphyseodesis and rodding for early onset scoliosis. Clinical Anatomy. 1990;3:241.
-
- Grivas TB, Webb JK, Burwell RG. The effects of epiphyseodesis and rodding for early onset scoliosis. J Bone Joint Surg. 1991;73B:32–33.
-
- Grivas TB, Webb JK, Burwell RG. Proceedings of the 25th Annual Meeting of the Scoliosis Research Society. Honolulu, Hawaii, USA; Progressive infantile idiopathic scoliosis: a comparison of three methods and the derotation of a combined procedure; p. 73. 23–27 September 1990.
-
- Dansereau J, Stokes IAF, Moreland MS. Radiographic reconstruction of 3D human rib cage. In: Stokes IAF, Pekelsky JR, Moreland MS, editor. Surface Topography and Spinal Deformity. Stuttgart: Gustav Fischer; 1987. pp. 67–76.
-
- Emans J. Proceedings of the the 39th Annual Meeting of the Scoliosis Research Society. Buenos Aires, Argentina; Earlier and more extensive thoracic fusion is associated with diminished pulmonary function outcomes after spinal fusion of 4 or more thoracic spinal segments before age 5. September 6–9, 2004.
LinkOut - more resources
Full Text Sources
