

Structural organization of choroidal colobomas of young and adult patients and mechanism of retinal detachment
- PMID: 17057813
- PMCID: PMC1447584
Structural organization of choroidal colobomas of young and adult patients and mechanism of retinal detachment
Abstract
Purpose: In colobomatous eyes, the risk of retinal detachment increases with age. This study elucidates the anatomic conditions and pathologic process of retinal detachment associated with colobomas.
Methods: The records, including histologic slides, of 14 children (1 day to 17 months old) and 7 adults (17 to 78 years old) with colobomas were examined.
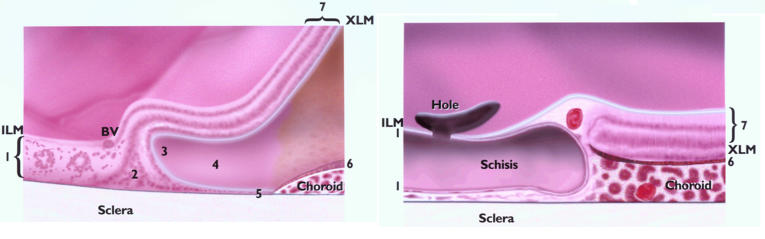
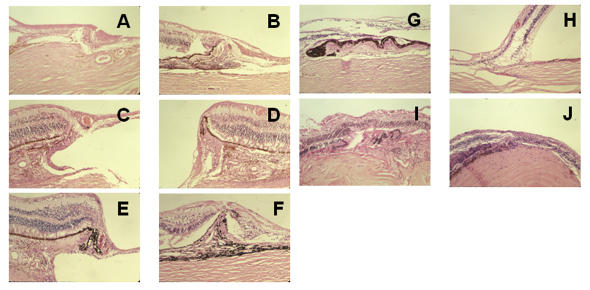
Results: In children, colobomas were associated with lethal malformations. The extracolobomatous inner retinal layers extended centrally, forming the intercalary membrane. Duplication of the outer retinal layers and a horizontal shift of Müllerian glia created a triangle and a locus minoris resistentiae adjacent to the laterally displaced pigment epithelium. Part of the locus was an incomplete layer of photoreceptors excluding Müllerian glia. In adults, atrophy of the intercalary membrane, manifested as central schisis, thinning of the neuroepithelium, and hole formation, was related to a paucity of blood vessels within and underneath the intercalary membrane and the size of colobomas. The margins featured blood vessels, pigment epithelial hypertrophy, and choroidal and scleral thickening in a compact, intertwined arrangement.
Conclusions: Glial atrophy, schisis, and hole formation in the intercalary membrane and separation of the locus minoris resistentiae from the pigment epithelium can disrupt barriers to fluid flow and set the stage for rhegmatogenous retinal detachment. That process is exacerbated by scleral ectasia, increasing vitreous traction at the margin, and retinovascular ischemia within the intercalary membrane. A vascularized, compact margin resembling a laser barrier, found predominantly in adults, may protect against retinal detachment.
Figures
References
-
- Von Ammon. Anatomische Untersuchung von Coloboma bulbi. Z Ophthalmol 1830: I.
-
- Jesberg D, Schepens C. Retinal detachment associated with coloboma of the choroid. Arch Ophthalmol. 1961;65:163–173. - PubMed
-
- Schepens CL. Retinal Detachment and Allied Diseases Vol 2. Philadelphia: WB Saunders; 1983:615–617.
-
- Hannover A. Cited by Hess C. Zur Pathogenese des Microphthalmus. Archiv Ophthalmol. 1888;34:162.
-
- Hannover A. Funiculus sclerae. Séance de L’academie des sciences danoise. 8. XII. 1876.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
