

Perifoveal vitreous detachment and its macular complications
- PMID: 17057817
- PMCID: PMC1447588
Perifoveal vitreous detachment and its macular complications
Abstract
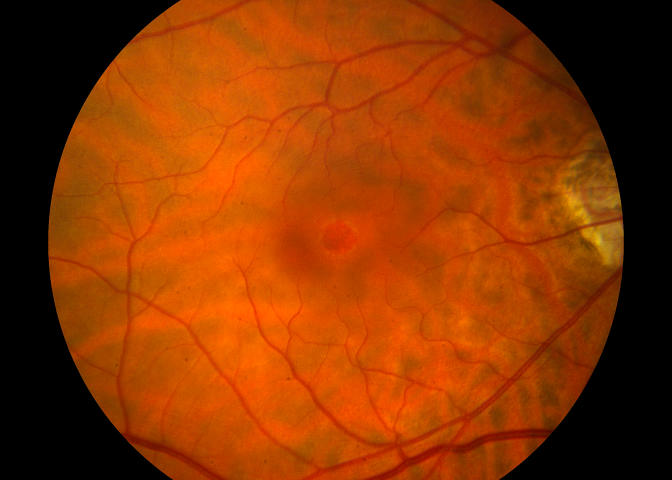
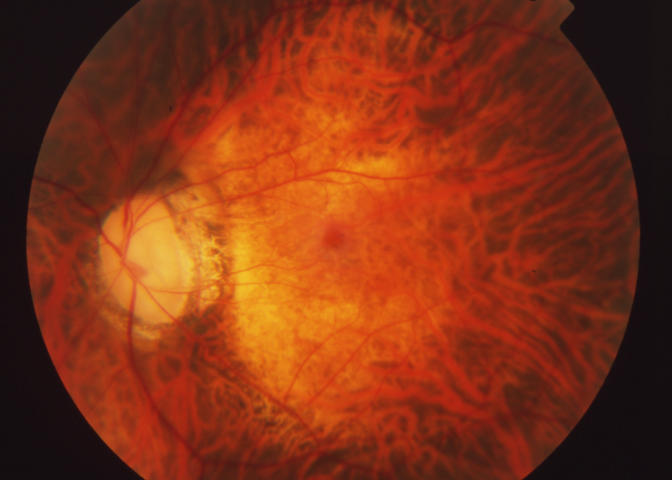
Purpose: To evaluate the vitreoretinal relationship in eyes with idiopathic macular disorders putatively caused by vitreomacular traction associated with early stages of age-related posterior vitreous detachment (PVD).
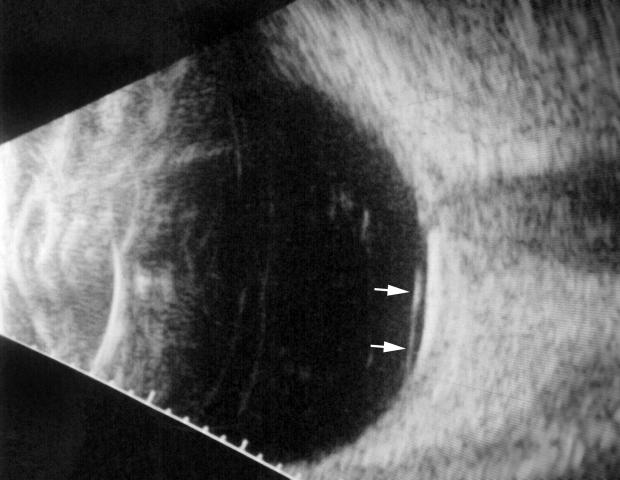
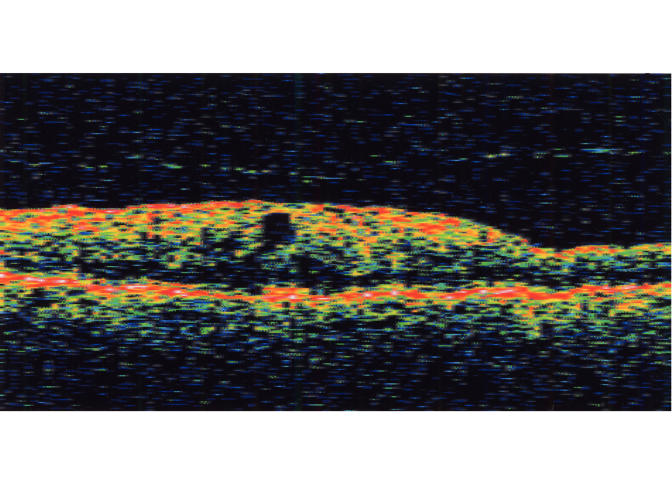
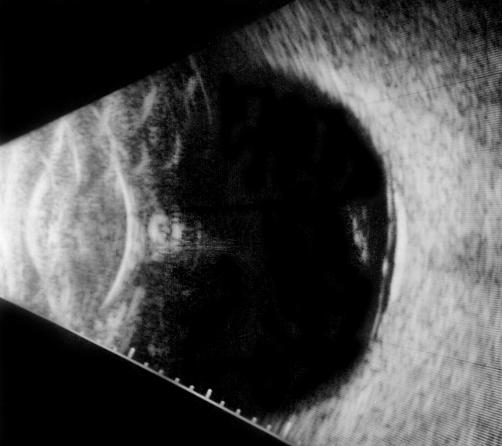
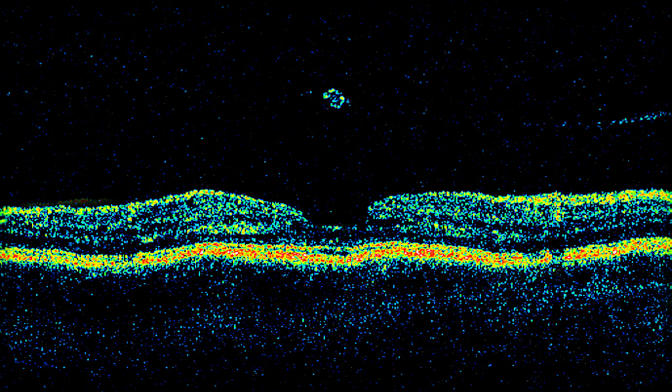
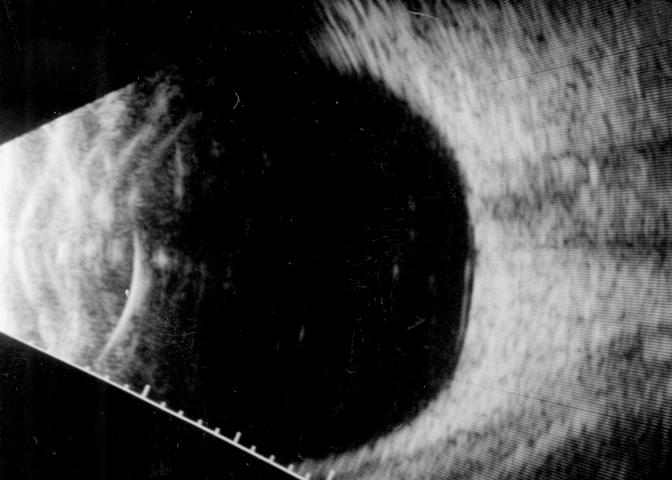
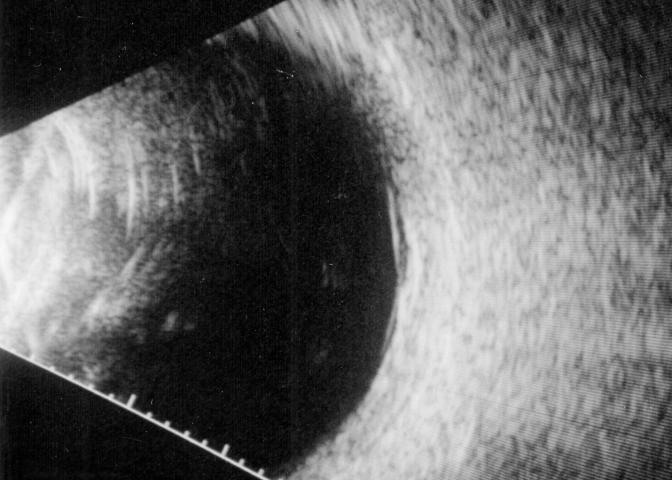
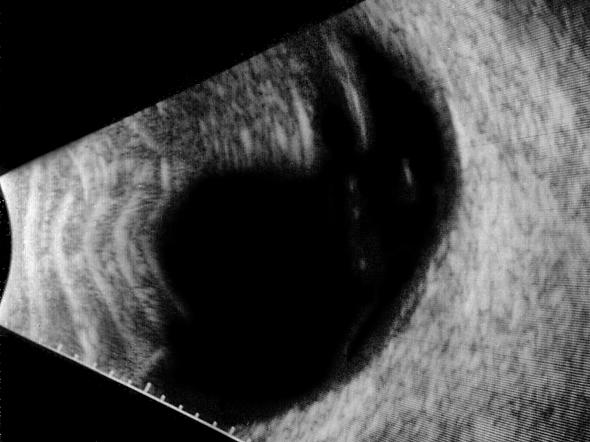
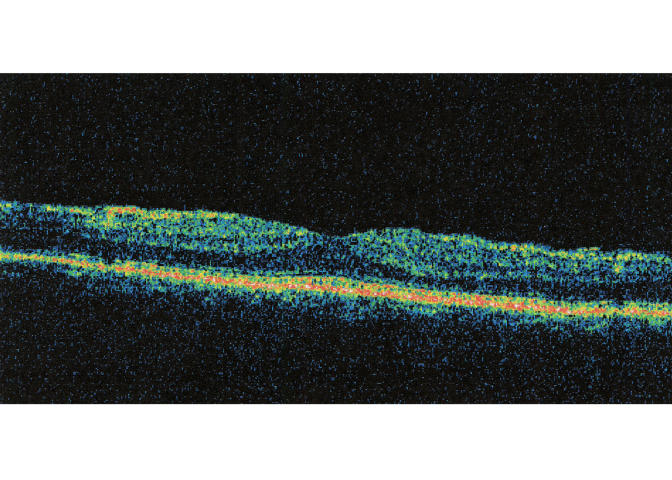
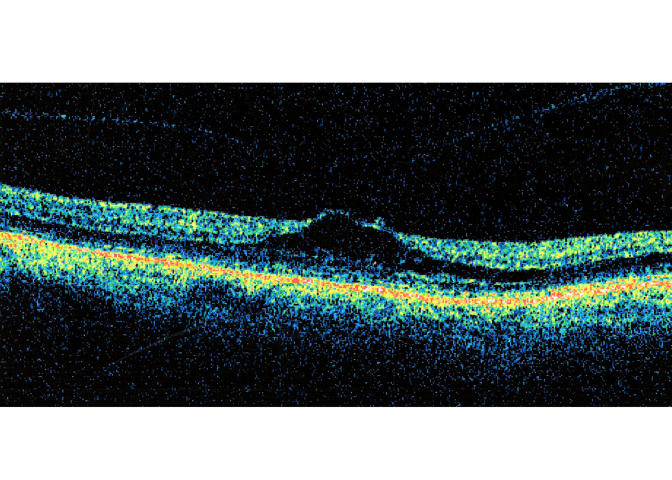
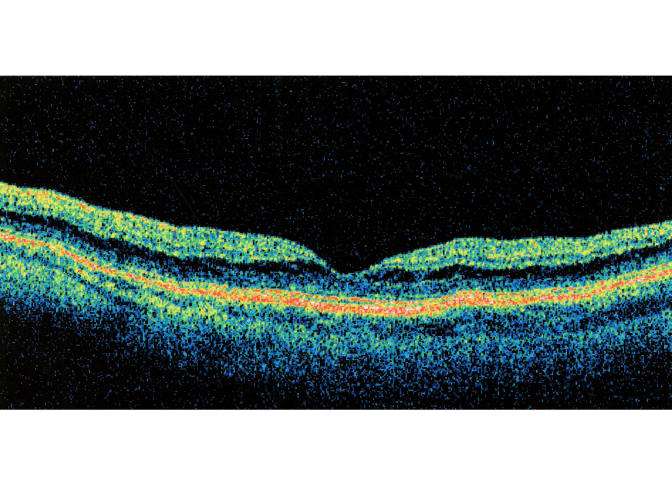
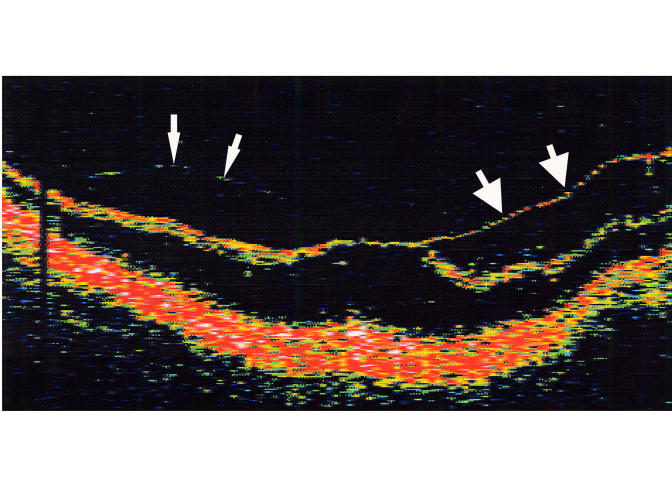
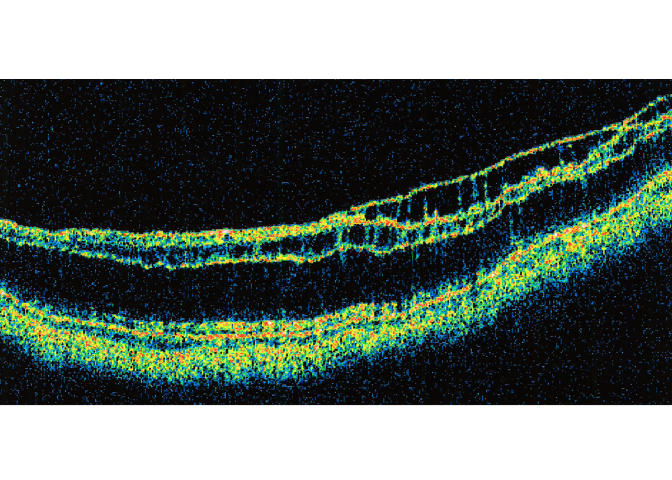
Methods: Retrospective observational case series of 43 eyes of 40 patients diagnosed with one of several idiopathic vitreomacular conditions. Included patients had no biomicroscopic evidence for complete PVD on presentation and underwent a specific clinical assessment of the vitreoretinal relationship. Affected eyes were evaluated with slit-lamp biomicroscopy, B-scan ultrasonography, optical coherence tomography, and/or intraoperative examination of the posterior hyaloid.
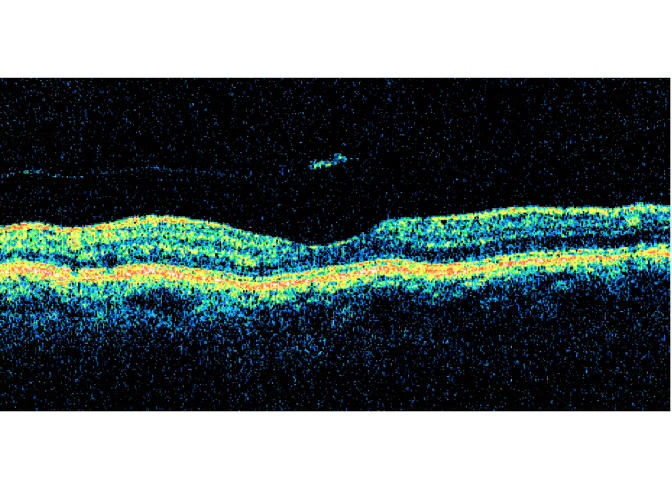
Results: By one or more examination techniques, 41 (95.3%) of the 43 study eyes had evidence of vitreous detachment from the perifoveal macular region and the remaining two eyes had complete PVD. When measurable, the size of the vitreomacular adhesion varied by diagnosis. Of 31 eyes with perifoveal vitreous detachment seen in follow-up, only three (9.7%) showed progression to complete PVD over an average preoperative or total follow-up period of 30.0 months (range, 2 to 237 months). Surgical or spontaneous separation of the residual vitreomacular adhesion in 16 eyes was followed in 15 (93.8%) by partial or complete resolution of the symptoms and signs of macular traction.
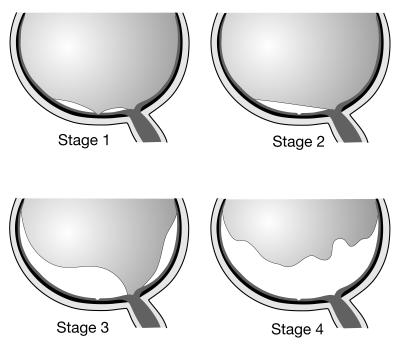
Conclusions: Age-related PVD appears to be an insidious, chronic event that begins in the perifoveal macula and evolves over a prolonged period of time prior to vitreopapillary separation. Though usually asymptomatic, its early (perifoveal) stages may be complicated by one of several macular pathologies, determined in part by the size of the residual vitreomacular adhesion.
Figures
























References
-
- Sebag J. The Vitreous: Structure, Function, and Pathobiology. New York: Springer-Verlag; 1989:80–95.
-
- Jaffe NS. Complications of acute posterior vitreous detachment. Arch Ophthalmol. 1968;79:568–571. - PubMed
-
- Foos RY, Wheeler NC. Vitreoretinal juncture: synchysis senilis and posterior vitreous detachment. Ophthalmology. 1982;89:1502–1512. - PubMed
-
- Eisner G. Posterior vitreous detachment. Klin Monatsbl Augenheilkd. 1989;194:389–392. - PubMed
-
- Balazs EA, Denlinger JL. Aging changes in the vitreous. In: Sekuler R, Kline D, Dismukes K, eds. Aging and Human Visual Function. New York: Liss; 1982:45–57.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
