

Discrepancies in the diagnosis of intraductal proliferative lesions of the breast and its management implications: results of a multinational survey
- PMID: 17058097
- PMCID: PMC1888715
- DOI: 10.1007/s00428-006-0245-y
Discrepancies in the diagnosis of intraductal proliferative lesions of the breast and its management implications: results of a multinational survey
Abstract
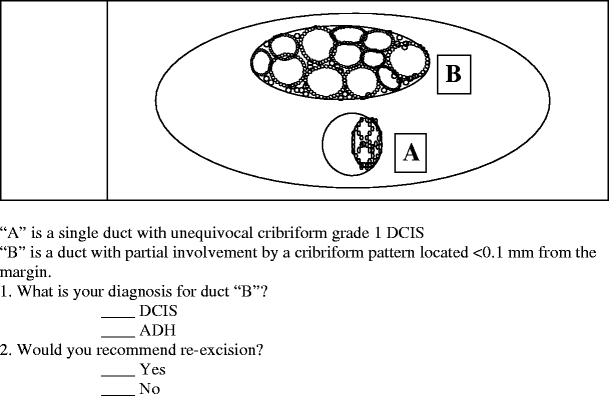
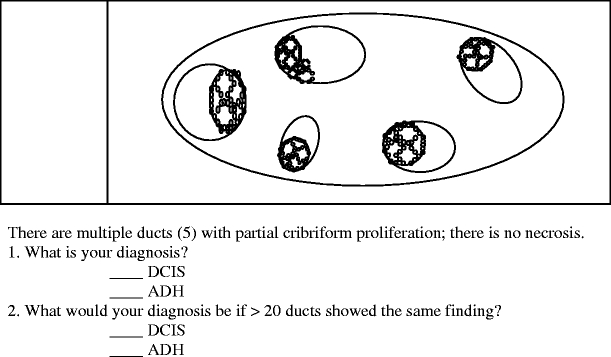
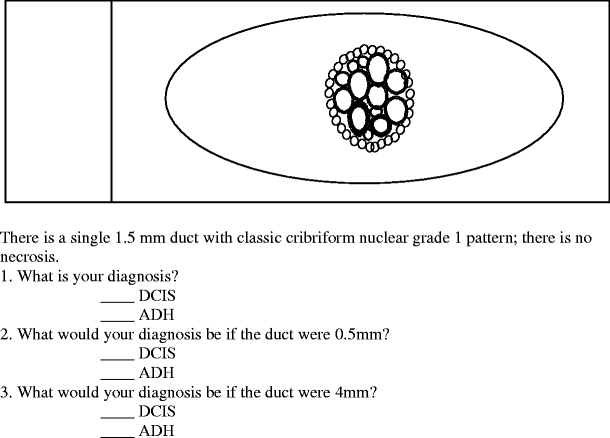
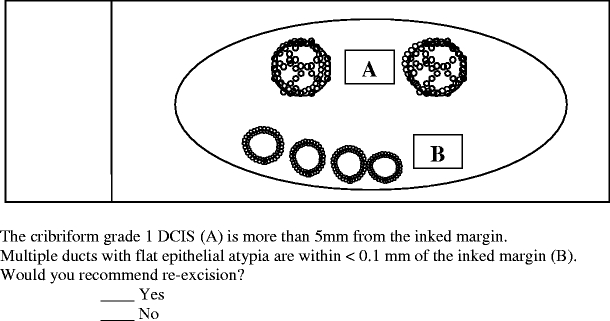
To measure discrepancies in diagnoses and recommendations impacting management of proliferative lesions of the breast, a questionnaire of five problem scenarios was distributed among over 300 practicing pathologists. Of the 230 respondents, 56.5% considered a partial cribriform proliferation within a duct adjacent to unequivocal ductal carcinoma in situ (DCIS) as atypical ductal hyperplasia (ADH), 37.7% of whom recommended reexcision if it were at a resection margin. Of the 43.5% who diagnosed the partially involved duct as DCIS, 28.0% would not recommend reexcision if the lesion were at a margin. When only five ducts had a partial cribriform proliferation, 35.7% considered it as DCIS, while if >or=20 ducts were so involved, this figure rose to 60.4%. When one duct with a complete cribriform pattern measured 0.5, 1.5, or 4 mm, a diagnosis of DCIS was made by 22.6, 31.3, and 94.8%, respectively. When multiple ducts with flat epithelial atypia were at a margin, 20.9% recommended reexcision. Much of these discrepancies arise from the artificial separation of ADH and low-grade DCIS and emphasize the need for combining these two under the umbrella designation of ductal intraepithelial neoplasia grade 1 (DIN 1) to diminish the impact of different terminologies applied to biologically similar lesions.
Figures
References
-
- Arpino G, Laucirica R, Elledge RM (2005) Premalignant and in situ breast disease: biology and clinical implications. Ann Intern Med 143(6):446–457 - PubMed
-
- Ashikari R, Huvos AG, Snyder RE, Sharma R, Kirch R, Schottenfeld D (1980) A clinicopathologic study of atypical lesions of the breast further follow up. Pathol Res Pract 166:481–490 - PubMed
-
- Azzopardi JG (1979) Problems in breast pathology. Saunders, Philadelphia - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
