

Angioedema without urticaria: a large clinical survey
- PMID: 17060655
- PMCID: PMC1609157
- DOI: 10.1503/cmaj.060535
Angioedema without urticaria: a large clinical survey
Abstract
Background: Angioedema without major urticarial flares (hives) is poorly understood. Its causes are diverse, and little is known about its pathogenic mechanisms. We report on our 11 years of experience with this condition and propose a classification of patients affected by angioedema unaccompanied by urticaria.
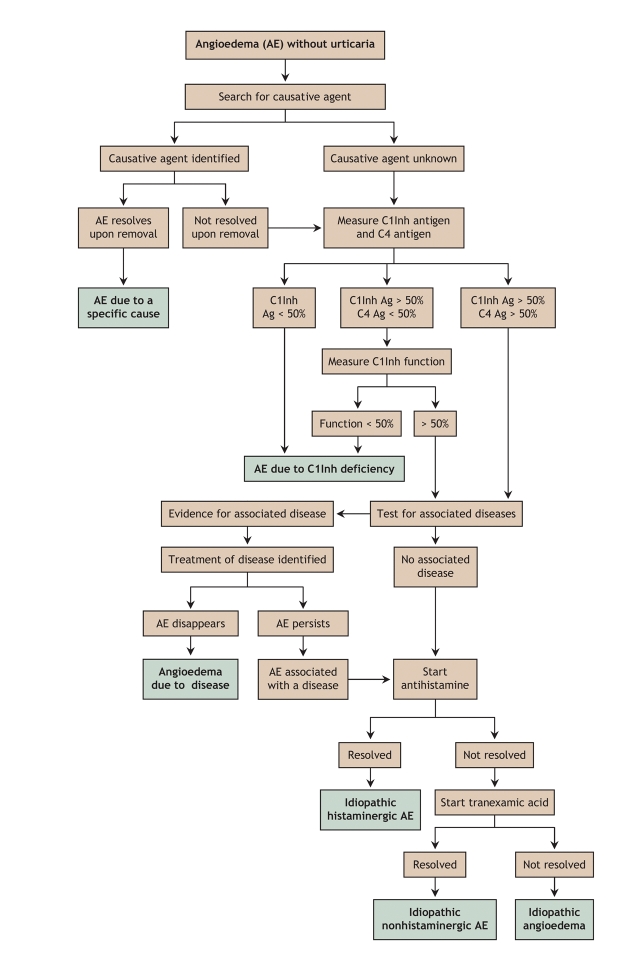
Methods: From 1993 through 2003 at our outpatient clinic, 929 consecutive patients were examined for recurrent angioedema unaccompanied by urticaria. A detailed history was taken to identify known causes of angioedema, with special attention to external allergenic agents. Each patient underwent a complete physical examination, routine laboratory tests (blood cell count, protein electrophoresis, erythrosedimentation rate, examination of stool for ova and parasites, pharyngeal and urine cultures, sinus and dental radiography, and measurements of antitissue autoantibodies and rheumatoid factor in plasma), and complement parameters (C1 inhibitor, C4 and C1q). Further testing was done when pertinent, based on clinical findings. When all results were negative, response to H1-antihistamine was considered.
Results: Angioedema could not be classified in 153 patients who were lost to follow-up (16.4%). Among the 776 cases with adequate data, these types of angioedema were identified: 124 (16%) related to external agents such as a drug, insect bite or foodstuff; 85 (11%) related to treatment with angiotensin-converting enzyme inhibitor; 55 (7%) associated with an autoimmune disease or infection; and 197 (25%) caused by C1 inhibitor deficiency. In the other 315 cases (41%), the etiology was undiscovered: 254 cases (33% of the study sample) were idiopathic histaminergic; 40 (5%) were idiopathic nonhistaminergic; and 21 (3%) had other causes of peripheral or generalyzed edema.
Interpretation: Our data indicated that angioedema without urticaria could be classified according to specific clinical and pathogenic characteristics, and we have suggested a work-up for patients experiencing this condition.
Figures
Comment in
-
Angioedema and the Canadian Network of Rare Blood Disorder Organizations: extending the Canadian hemophilia care model.CMAJ. 2006 Oct 24;175(9):1083. doi: 10.1503/cmaj.061236. CMAJ. 2006. PMID: 17060658 Free PMC article. No abstract available.
References
-
- Friedmann PS. Assessment of urticaria and angio-oedema. Clin Exp Allergy 1999; 29 (Suppl 3):109-12 [discussion 113-5]. - PubMed
-
- Grattan C, Powell S, Humphreys F. Management and diagnostic guidelines for urticaria and angio-oedema. Br J Dermatol 2001;144:708-14. - PubMed
-
- Cicardi M, Bisiani G, Cugno M, et al. Autoimmune C1 inhibitor deficiency: report of eight patients. Am J Med 1993;95:169-75. - PubMed
-
- Cicardi M, Zingale LC, Bergamaschini L, et al. Angioedema associated with angiotensin-converting enzyme inhibitor use: outcome after switching to a different treatment. Arch Intern Med 2004;164:910-3. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous